Seropositivity of borrelia burgdorferi s. L. In germany—an analysis across four german national cohort (nako) study sites
Seropositivity of borrelia burgdorferi s. L. In germany—an analysis across four german national cohort (nako) study sites"
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Lyme borreliosis (LB) is caused by the transmission of _Borrelia burgdorferi_ s.l. from ticks to humans. Climate affects tick abundance, and climate change is projected to promote
shifts in abundance in Europe, potentially increasing human exposure. We analyzed serum samples collected between the years 2014–2019 from German National Cohort (NAKO) participants at four
study sites (Augsburg, Berlin, Hanover, Münster) for immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies using an enzyme‐linked immunosorbent assay (ELISA) and line blot immunoassay
as confirmatory test for positive and equivocal ELISA samples. We reported crude and weighted seropositivity proportions for local estimates. We used mixed model analysis to investigate
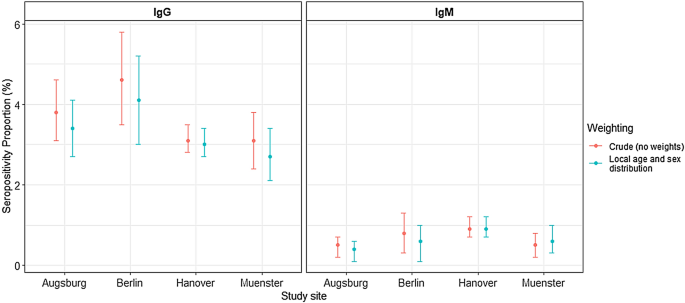
associated factors, such as age, sex, migration background, or animal contacts. We determined the serostatus of 14,207 participants. The weighted seropositivity proportions were 3.4% (IgG)
and 0.4% (IgM) in Augsburg, 4.1% (IgG) and 0.6% (IgM) in northern Berlin, 3.0% (IgG) and 0.9% (IgM) in Hanover, and 2.7% (IgG) and 0.6% (IgM) in Münster. We found higher odds for IgG
seropositivity with advancing age (_p_ < 0.001), among males compared to females (_p_ < 0.001) and reduced odds among participants with migration background compared to those without
(_p_ = 0.001). We did not find evidence for an association between serostatus and depression, children within the household, or animal contact, respectively. We found low seropositivity
proportions and indications of differences across the study locations, although between-group comparisons did not yield significant results. Comparisons to earlier research are subject to
important limitations; however, our results indicate no major increases in seropositivity over time. Nevertheless, monitoring of seropositivity remains critical in light of potential
climate-related _Borrelia_ exposure. SIMILAR CONTENT BEING VIEWED BY OTHERS DETECTION OF _BORRELIA BURGDORFERI_ ANTIGENS IN TISSUES AND PLASMA DURING EARLY INFECTION IN A MOUSE MODEL Article
Open access 30 August 2021 TICK-BORNE ENCEPHALITIS VIRUS SEROPREVALENCE AND INFECTION INCIDENCE IN SWITZERLAND, 2020–2021 Article Open access 11 March 2025 CORRELATION BETWEEN COVID-19
SEVERITY AND PREVIOUS EXPOSURE OF PATIENTS TO _BORRELIA_ SPP. Article Open access 24 September 2022 INTRODUCTION In Europe, Lyme borreliosis (LB) is the most frequent tick-borne disease
caused by _Borrelia burgdorferi_ sensu lato (_B. burgdorferi_ s.l.). Climatic factors affect the geographical spread of _Ixodes ricinus (I. ricinus)_, the primary vector of _B. burgdorferi_
s.l. in Europe1. Due to climate change-related temperature increases and humidity alterations, _I. ricinus_ expanded its territory while also showing prolonged seasonal activity2, implying
an increased potential risk for human exposure to ticks. Especially in central and northern Europe, reported LB cases have increased within the past two decades3. However, LB is a notifiable
disease in selected, but not all European countries4. In Germany, LB is partially notifiable in nine of sixteen federal states; notification data from these states indicate a varying but
steady incidence by region for the years 2013–2017, ranging from 26 to 41 cases per 100,000 persons5, while nation-wide health insurance data from 2019 indicated an incidence of 179 cases of
LB per 100,000 insured persons in Germany6. Two recent local serological surveys conducted in Hanover, Northern Germany (2014–2018)7, and in Bonn in Western Germany (2018–2020)8,
respectively, found no increases in seropositivity proportions compared to earlier investigations (1997–1999 and 2008–2011, respectively)9, despite increases in tick density in at least one
German region (Siebengebirge near Bonn). The data for Hanover is included in this work with a different research focus. Our work aims (1) to estimate the local seropositivity proportion of
antibodies against _B. burgdorferi_ s.l. among the general population of four different regions in Germany based on a nation-wide population-based cohort study (Augsburg in southern, Berlin
North in Eastern-, Hanover in Northern-, and Münster in Western Germany) with—for the first time—high accuracy due to large sample size; (2) to compare seropositivity using identical age-
and sex population weights; and (3) to investigate risk factors for seropositivity across regions. The data create a base for future comparisons regarding potentially increasing human _B.
burgdorferi_ s.l. exposure and enable investigations of seroconversion and –reversion within a large and ongoing cohort. METHODS The German National Cohort (NAKO) is a prospective
population-based cohort study with 205,415 baseline participants examined across 18 study sites10. All potential NAKO-participants were randomly drawn from population registries. Subjects
were eligible for participation when aged between 20 and 69 years at sampling date, provided written informed consent, had their primary residence within a regionally limited catchment area
corresponding to the responsible NAKO study site, and were of sufficient health for study participation on site. Participants aged 40 years and above were oversampled. Detailed information
is provided by Peters et al.10. All participants provided written informed consent. In our investigation, we randomly selected baseline serological samples from the urbanized sites Augsburg,
Berlin North, Münster, and used all eligible samples from Hanover. The Hanover data were reported before7 with a different research focus. We performed stratified random sampling for the
three other study sites after restricting to those with: available data for risk factor evaluation (if possible), focusing on a target distribution of 50% males and a distribution of age
groups corresponding to the original NAKO recruitment, i.e., an oversampling of the age groups ≥ 40 years. A laboratory (DIN EN ISO accredited, ISO 9001 certified) screened all samples for
immunoglobulin G (IgG) and immunoglobulin M (IgM) _B. burgdorferi_ s.l. antibodies using an enzyme‐linked immunosorbent assay (ELISA). Positive and equivocal ELISA samples underwent line
blot immunoassay for confirmation (test kit information: Table S1). In the primary analysis, we considered a sample with positive or equivocal ELISA and positive line blot result as a
seropositive (classification according to the microbiologic-infectiologic quality standard MIQ12). For the secondary analysis to allow comparability with two previous studies, we considered
a positive ELISA sample with subsequent positive or equivocal line blot or an equivocal ELISA with a positive line blot as positive 9. We classified each sample for IgG and IgM serostatus
based on these two schemes. To estimate general population seropositivity, we weighted our sample with the respective local age and sex distribution based on the 2020 update of the 2011
census (www.destatis.de). For comparison with earlier estimates, we additionally weighted by the age- and sex distributions of the underlying study populations of the German National Health
Interview and Examination Survey 1998 (BGS98, 1997–1999) and the German Health Interview and Examination Survey for Adults (DEGS, 2008–2011)9. Due to low total number of IgM-positive
samples, we restricted further analyses to IgG antibodies. We used the χ2-test for trend in proportions to investigate a potential seropositivity trend with age, and with increasing
education level. Then, we used the χ2-test (two-sided) to test for differences in German standard-population-weighted (2020 update of the 2011 census) seropositivity proportions between the
study sites, and used post-hoc pairwise comparisons between the individual centers using the Fisher’s exact test (two-sided) with Bonferroni correction. To evaluate potential risk factors
for seropositivity, we used logistic mixed model analysis, with study centers as the clusters. We constructed models to estimate odds ratios (OR) for IgG seropositivity; in model 1, as a
function of sex, age, education level, migration background, depression (score ≥ 10 of the 9-question Patient Health Questionnaire, PHQ-9), children within the household; in model 2, as a
function of all variables from model 1 and additionally animal-related variables (having a particular pet vs. no pet) due to their restricted availability by NAKO design. We controlled for
education level and migration background in our models to add additional evidence to recent conflicting findings concerning the role of socioeconomic factors concerning seropositivity7, 8.
Due to the indication of a potential association of seropositivity with depressive symptomatology 7, we also added depression as control variable to obtain further insight. To provide
insights into potentially altered tick exposure with children living in the same household, e.g., by altered outdoor activities8, we added this variable to our models as control variable. We
considered a significance level of 5% to determine statistical significance. All analysis and visualization was conducted in R version 4.1.2. We used the package “survey” to apply weights,
“gtsummary” to support table creation, “ggplot” for visualization, and the glmer()-function from “lme4” to fit the mixed model. Finally, we used the “DHARMa”-package for further inspection
of the model, e.g., residual analysis. ETHICS APPROVAL The Bavarian Medical Association (“Bayerische Landesärztekammer”) approved all NAKO-related human examinations as the central ethics
committee [13023, 13031]. Local medical associations additionally approved the examinations. Our study respects all national laws and the 1975 Declaration of Helsinki in the current version.
RESULTS Blood samples of 14,207 participants were available for our analysis. The participants were aged 20–74 years, with a median age of 50; 50.0% were male, 55.6% reported high education
according to ISCED97, and 18.0% had a migration background. The overall crude IgG-seropositivity proportion was 3.4%. Generally, we found an increasing trend concerning crude seropositivity
with advancing age (_p_ < 0.001); however, differences were only significant when comparing the older age group 60–69 (5.2%; 95% confidence interval (CI) 4.5–5.9%) to the younger age
group 20–29 (2.6%; 95%-CI 1.8–3.5%) (Table 1). Overall, males had higher seropositivity (4.8%; 95%-CI 4.3–5.3%) than females (2.0%; 95%-CI 1.6–2.3%). Seropositivity increased with education:
1.3% (95%-CI 0.0–2.2%) in the lowest group and 3.9% (95%-CI 3.4–4.3) in the highest education group across all sites (p < 0.001). Participants without a migration background had higher
seropositivity (3.7%; 95%-CI 3.4–4.0%) than those with a migration background (2.0%; 95%-CI 1.5—2.6). We did not observe differences in seropositivity between participants with depression
(3.0%; 95%-CI 2.2–3.8%) or without depression (3.5%; 95%-CI 3.1–3.8%) and between participants with pets (dogs: 2.3%; 95%-CI 0.8–3.8%) compared to those without pets (3.9%; 95%-CI 3.1–4.8%).
Local population-weighted point seropositivity varied by location (Fig. 1, Table S2). Participants from Berlin had the highest weighted IgG seropositivity proportion (4.1%, 95%-CI
3.0–5.2%), while those from Münster had the lowest weighted proportion (2.7%, 95%-CI 2.1–3.4). The CI of seropositivity proportions overlapped between the four sites. However, the χ2-test
indicated overall differences in proportions for estimates weighted by nation-wide age and sex population proportions from 2020 (_p_ = 0.04). The pairwise comparisons with Fisher's
exact test did not yield significant results at the 95% significance level. Table S3 reports weighted seropositivity using the age- and sex distribution of earlier studies9. From logistic
mixed-model analysis, we found that every 10-year increase in age was associated with 1.26-fold (95%-CI 1.16–1.38) the odds for IgG-seropositivity (Table 2). Men had 2.54 times (95%-CI
2.05–3.13) the odds of being IgG-seropositive compared to females. Participants with a migration background had 0.56 (95%-CI 0.41–0.78) times the odds for a positive IgG-serostatus compared
to participants with no migration background. We did not find evidence for an association of IgG serostatus with education level, depression on a binary scale (PHQ-9), children within the
household (any versus none), or any current or previous animal contacts, respectively. DISCUSSION We conducted the largest-ever German multi-center serological survey for _B. burgdorferi_
s.l. in Germany. We compared seropositivity estimates of four German regions representing the four cardinal directions. The crude proportion of seropositive participants slightly varied by
study location. We estimated the local seropositivity to lie between 4.1% in Berlin (95%-CI 3.0–5.2%) and 2.7% in Münster (95%-CI 2.1–3.4). The comparison of our findings to earlier studies
is subject to critical limitations due to differences in the sampling methodology. We could not account for factors such as the degree of rurality or other living conditions. However, when
classifying our samples like in9 and weighting them by age and sex for comparability to two earlier studies9 based on BGS98 and DEGS, we did not find any indication for relevant increases in
seropositivity. Seropositivity in Augsburg was lower in our study when compared to BGS98 (6.1%, 95%-CI 5.1–7.0% vs. 10.4%, 95%-CI 7.5–13.4%) and DEGS estimates (6.5%, 95%-CI 5.5–7.4% vs.
12.1, 95%-CI 8.8–15.4%) for Bavaria. Seropositivity for Hanover was comparable with Lower-Saxony estimates in BGS98 (4.9%, 95%-CI 4.5–5.4% vs. 7.4%, 95%-CI 5.1–9.6%), but lower when compared
to DEGS (5.3%, 95%-CI 4.8–5.8% vs. 9.1%, 95%-CI 6.7–11.4%). For northern Berlin, seropositivity was comparable to BGS98 jointly reported estimates for Brandenburg, Mecklenburg-Vorpommern,
and Saxony-Anhalt (5.0%, 95%-CI 3.8–6.3% vs. 7.2%, 95%-CI 5.8–8.7%). Similarly, seropositivity was comparable when comparing northern Berlin seropositivity estimates to DEGS estimates (5.6%,
95%-CI 4.3–6.9% vs. 9.3%, 95%-CI 6.8–11.9). When considering the seropositivity proportions for Münster, we found a similar seropositivity proportion compared to earlier BGS98-estimates for
North Rhine-Westphalia (5.2%, 95%-CI 4.3–6.1% vs. 7.4%, 95%-CI 5.1–9.6). However, seropositivity was lower than DEGS estimates (5.5%, 95%-CI 4.5–6.4 vs. 9.1%, 95%-CI 6.7–11.4). All four
study sites recruited participants from predominantly urban areas, which may have resulted in reduced seropositivity proportion compared to earlier investigations, which included a higher
proportion of rural participants. Within DEGS, participants living in municipalities with less than 5000 inhabitants had twice the chance for being seropositive compared with those with more
than 100,000 inhabitants11, potentially due to higher exposure to green-space areas and, therefore, ticks. Notification data from Bavaria and Berlin supports this by showing that, compared
to the surrounding region, Berlin and Augsburg had lower incidences5. Our results confirm advancing age and male sex as risk factors for positive antibody detection. As found in earlier
studies, adults with a migration background were less likely to be seropositive11, 12. We did not find conclusive evidence for an association between educational level, current depression
(PHQ-9 score ≥ 10), or previous or current animal contact with serostatus, respectively. Our results from multivariable modelling concerning educational level are in line with previous
studies, which also found no association between socio-economic status and serostatus9, but opposes recent findings from a population-based cohort in central Bonn, in which highly educated
individuals had higher chances for positive serostatus compared to individuals with medium-level education8. The conflicting findings might be explainable by the availability or use of
different outdoor spare time activities in different urban regions. Additional investigations including higher proportions of participants with lower and intermediate education are required
to complement this discussion. In contrast to a previous study using the original PHQ-9-scores as a proxy for depression diagnosis7, we did not find evidence for an association between
serostatus and depression on a binary scale. Our findings did not support an association between animal contacts and seropositivity, which is in line with earlier findings among adults11,
but contrasts a previous finding12, which found higher chances for seropositivity among children living in households with any pet vs. no pet or with a cat vs. no cat, respectively. Our work
has several limitations. Most samples considered in our regression analysis originate from the study center in Hanover. Hence, our analysis is predominantly driven by this single-site data.
Furthermore, the use of test kits with differing specificity, sensitivity, and considered _Borrelia_ strains between the studies hamper the comparability of seropositivity proportions of
our study with previous analyses. A long-term cohort like NAKO can overcome this in the future by providing the basis for a harmonized longitudinal seropositivity analysis. The small number
of seropositive individuals in the low education group and the groups of individuals with animals in the household may have resulted in low statistical power and, thus, the inability to
identify a potential association in the regression models. In conclusion, we found low seropositivity across four study locations across Germany, with minor indications of differences
between sites. Our seropositivity estimates of the years 2014–2019 for four predominantly urban regions correspond to previous estimates for 1997–1999 and 2008–2011, respectively, indicating
no considerable increases of seropositivity over time. However, comparisons to earlier estimates suffer from limitations. Even in urbanized regions, potential climate-change-related shifts
in tick exposure may increase infections and, therefore, non-urgent follow-up may be conducted in future waves of the NAKO cohort study. Our findings underpin previously suggested risk
factors for seropositivity, with advancing age and male sex as the most critical risk factors. Migration status appears as an additional factor of lower seropositivity since many persons
migrating to Germany may come from countries with little or no _Borrelia_ exposure. DATA AVAILABILITY The German National Cohort (NAKO) data is not openly available due to data protection
measures. However, scientists can apply for data access following the official usage regulations and upon formal request to the NAKO use and access committee (https://transfer.nako.de/).
REFERENCES * Steere, A. C. _et al._ Lyme borreliosis. _Nat. Rev. Dis. Prim._ 2, 16090. https://doi.org/10.1038/nrdp.2016.90 (2016). Article PubMed Google Scholar * Estrada-Peña, A. &
Fernández-Ruiz, N. A retrospective assessment of temperature trends in northern Europe reveals a deep impact on the life cycle of _Ixodes ricinus_ (Acari: Ixodidae). _Pathogens_
https://doi.org/10.3390/pathogens9050345 (2020). Article PubMed PubMed Central Google Scholar * Vandekerckhove, O., de Buck, E. & van Wijngaerden, E. Lyme disease in Western Europe:
An emerging problem? A systematic review. _Acta Clin. Belg._ 76, 244–252. https://doi.org/10.1080/17843286.2019.1694293 (2021). Article PubMed Google Scholar * Steinbrink, A., Brugger,
K., Margos, G., Kraiczy, P. & Klimpel, S. The evolving story of _Borrelia burgdorferi_ sensu lato transmission in Europe. _Parasitol. Res._ 121, 781–803.
https://doi.org/10.1007/s00436-022-07445-3 (2022). Article PubMed PubMed Central Google Scholar * Enkelmann, J. _et al._ Incidence of notified _Lyme borreliosis_ in Germany, 2013–2017.
_Sci. Rep._ 8, 14976. https://doi.org/10.1038/s41598-018-33136-0 (2018). Article ADS CAS PubMed PubMed Central Google Scholar * Akmatov, M. K. _et al._ Epidemiology of _Lyme
borreliosis_ based on outpatient claims data of all people with statutory health insurance, Germany, 2019. _Euro Surveill._ https://doi.org/10.2807/1560-7917.ES.2022.27.32.2101193 (2022).
Article PubMed PubMed Central Google Scholar * Hassenstein, M. J. _et al._ Seroepidemiology of _Borrelia burgdorferi_ s.l. among German national cohort (NAKO) participants, Hanover.
_Microorganisms._ https://doi.org/10.3390/microorganisms10112286 (2022). Article PubMed PubMed Central Google Scholar * Coors, A. _et al._ Regional seropositivity for _Borrelia
burgdorferi_ and associated risk factors: findings from the Rhineland Study, Germany. _Parasit. Vectors_ 15, 241. https://doi.org/10.1186/s13071-022-05354-z (2022). Article CAS PubMed
PubMed Central Google Scholar * Woudenberg, T. _et al._ Dynamics of _Borrelia burgdorferi_-specific antibodies: Seroconversion and seroreversion between two population-based,
cross-sectional surveys among adults in Germany. _Microorganisms_ https://doi.org/10.3390/microorganisms8121859 (2020). Article PubMed PubMed Central Google Scholar * Peters, A. _et al._
Framework and baseline examination of the German National Cohort (NAKO). _Eur. J. Epidemiol._ 37, 1107–1124. https://doi.org/10.1007/s10654-022-00890-5 (2022). Article CAS PubMed PubMed
Central Google Scholar * Wilking, H., Fingerle, V., Klier, C., Thamm, M. & Stark, K. Antibodies against _Borrelia burgdorferi_ sensu lato among Adults, Germany, 2008–2011. _Emerg.
Infect. Dis._ 21, 107–110. https://doi.org/10.3201/eid2101.140009 (2015). Article CAS PubMed PubMed Central Google Scholar * Dehnert, M. _et al._ Seropositivity of Lyme borreliosis and
associated risk factors: a population-based study in children and adolescents in Germany (KiGGS). _PLoS One_ 7, e41321. https://doi.org/10.1371/journal.pone.00413 (2012). Article ADS CAS
PubMed PubMed Central Google Scholar Download references FUNDING Open Access funding enabled and organized by Projekt DEAL. This project used German National Cohort (NAKO) data
(www.nako.de). NAKO is funded by the German Federal Ministry of Education and Research (BMBF), the Helmholtz Association, and federal states. Participating universities and institutes of the
Leibniz Association provided additional funding. Funding references: 01ER1301A/B/C and 01ER1511D. MJH receives a scholarship from the Life Science Stiftung (LSS) to promote science and
research. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department for Epidemiology, Helmholtz Centre for Infection Research (HZI), Braunschweig, Germany Max J. Hassenstein, Yvonne Kemmling
& Stefanie Castell * PhD Programme “Epidemiology”, Braunschweig-Hannover, Germany Max J. Hassenstein * Max-Delbrueck-Center for Molecular Medicine in the Helmholtz Association (MDC),
Molecular Epidemiology Research Group, Berlin, Germany Tobias Pischon, Ilais Moreno Velásquez & Jürgen Janke * Max-Delbrueck-Center for Molecular Medicine in the Helmholtz Association
(MDC), Biobank Technology Platform, Berlin, Germany Tobias Pischon & Jürgen Janke * Berlin Institute of Health at Charité-Universitätsmedizin Berlin, Core Facility Biobank, Berlin,
Germany Tobias Pischon * Charité-Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität Zu Berlin, Berlin, Germany Tobias Pischon * Institute of
Epidemiology and Social Medicine, University of Münster, Münster, Germany André Karch & Henning Teismann * Institute of Epidemiology, Helmholtz Zentrum München–German Research Center for
Environmental Health (GmbH), Neuherberg, Germany Annette Peters, Alexandra Schneider & Sigrid Thierry * Chair of Epidemiology, Institute for Medical Information Processing, Biometry and
Epidemiology, Medical Faculty, Ludwig-Maximilians-Universität München, Munich, Germany Annette Peters * Department of RNA-Biology of Bacterial Infections, Helmholtz Institute for RNA-Based
Infection Research, Würzburg, Germany Tobias Kerrinnes * NAKO Studienzentrum, Klinik für Diagnostische und Interventionelle Radiologie und Neuroradiologie, Universitätsklinikum Augsburg,
Augsburg, Germany Sigrid Thierry * TWINCORE, Centre for Experimental and Clinical Infection Research, a Joint Venture of the Hannover Medical School and Helmholtz Centre for Infection
Research, 30625, Hannover, Germany Stefanie Castell Authors * Max J. Hassenstein View author publications You can also search for this author inPubMed Google Scholar * Tobias Pischon View
author publications You can also search for this author inPubMed Google Scholar * André Karch View author publications You can also search for this author inPubMed Google Scholar * Annette
Peters View author publications You can also search for this author inPubMed Google Scholar * Tobias Kerrinnes View author publications You can also search for this author inPubMed Google
Scholar * Henning Teismann View author publications You can also search for this author inPubMed Google Scholar * Alexandra Schneider View author publications You can also search for this
author inPubMed Google Scholar * Sigrid Thierry View author publications You can also search for this author inPubMed Google Scholar * Ilais Moreno Velásquez View author publications You can
also search for this author inPubMed Google Scholar * Jürgen Janke View author publications You can also search for this author inPubMed Google Scholar * Yvonne Kemmling View author
publications You can also search for this author inPubMed Google Scholar * Stefanie Castell View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS
Conceptualization: SC, MJH; Methodology: M.J.H., S.C., T.P.; Formal analysis: M.J.H.; Investigation: S.C., Y.K., A.K., T.P., A.P., H.T., S.T., J.J.; Data Curation: M.J.H.; Writing—Original
Draft: M.J.H.; Writing—Review & Editing: M.J.H., S.C., T.P., A.P., A.K., H.T., A.S., I.M.V., T.K.; Visualization: M.J.H.; Supervision: S.C.; Project administration: S.C.; Funding
acquisition: S.C., T.K. All authors reviewed the manuscript. CORRESPONDING AUTHOR Correspondence to Stefanie Castell. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no competing
interests. ADDITIONAL INFORMATION PUBLISHER'S NOTE Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. SUPPLEMENTARY
INFORMATION SUPPLEMENTARY INFORMATION. RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing,
adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons
licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise
in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the
permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints and
permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Hassenstein, M.J., Pischon, T., Karch, A. _et al._ Seropositivity of _Borrelia burgdorferi_ s.l. in Germany—an analysis across four German
National Cohort (NAKO) study sites. _Sci Rep_ 13, 21087 (2023). https://doi.org/10.1038/s41598-023-47766-6 Download citation * Received: 20 February 2023 * Accepted: 17 November 2023 *
Published: 30 November 2023 * DOI: https://doi.org/10.1038/s41598-023-47766-6 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable
link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative
Trending News
Lisa Tozzi – Rolling StoneLisa TozziExecutive Digital DirectorXemailLisa Tozzi is Rolling Stone’s Executive Digital Director. She oversees the dai...
AC/DC Reveal Retired Bassist Cliff Williams Will Return for Power Trip FestComebackAC/DC Reveal Retired Bassist Cliff Williams Will Return for Power Trip FestAhead of first concert since Septembe...
Chance the Rapper Takes Some Heat For His Latest FestivalTough QuestionsChance the Rapper Takes Some Heat For His Latest FestivalThe star from Chicago responds to criticism of h...
Coronation street spoilers: sally metcalfe's new look distracts fansSomeone else wrote: “#What the hell is Sally wearing on her head? #Corrie.” “Can’t stop looking at Sally’s beret #Corona...
Parents Oppose Lorbeer Official’s Ouster : Education: Differences between the junior high school principal and Pomona Unified administrators have appaA group of parents say they will ask the Pomona Unified School District board Tuesday to reinstate a controversial junio...
Latests News
Seropositivity of borrelia burgdorferi s. L. In germany—an analysis across four german national cohort (nako) study sitesABSTRACT Lyme borreliosis (LB) is caused by the transmission of _Borrelia burgdorferi_ s.l. from ticks to humans. Climat...
DiCicco Says It’s Time to Go HomeThe most successful coach in American soccer history, the coach who in the last five years led the U.S. women’s national...
DANA POINT - Los Angeles TimesThe City Council will consider donating $4,500 in grants and contributions to a number of local nonprofit organizations ...
Javascript support required...
Opinion: Rising economic burden on the urban working class widens rich-poor gapThe first urban commission in 1988 visualised development of cities by linking them with manufacturing and industrialisa...