Fracture fragment of the condyle determines the ramus height of the mandible in children with intracapsular condylar fractures treated conservatively
Fracture fragment of the condyle determines the ramus height of the mandible in children with intracapsular condylar fractures treated conservatively"
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT This study aimed to explore and impart understanding of bone remodelling in children with intracapsular fractures treated conservatively. Records of children (less than 12 years),
who sustained intracapsular fractures and treated conservatively, were retrieved consecutively for the period of March 2011 to February 2016. Data about age, gender, date of injury, dates of
admission and discharge, mechanism of trauma, location and pattern of fracture, other mandibular fractures, treatment methods and time of review were recorded and analysed. Image dates of
pre- and post-treatments, including date of review, were also recorded. A total of 22 patients complete their follow-up and show bone remodelling process. During their follow-up, all the
displaced condylar fragments fused with the ramus stump at the displaced position. Regardless of the type of conservative procedure, both treatments cannot promote the spontaneous fracture
reduction in patients with intracapsular condylar fractures. During follow-up, the absorption of the lateral process of the condyle after the closed treatment becomes close to the
‘horizontal absorption’, until the height (or articular surface) of the lateral condylar process dropped and aligned to the articular surface of the medial process. In children with
intracapsular condylar fractures, the fracture fragment of the condyle determines the ramus height of the mandible. Closed treatment cannot restore the fracture fragment. If the height of
the fracture fragments dropped remarkably, then open reduction and rigid internal fixation become more suitable. SIMILAR CONTENT BEING VIEWED BY OTHERS A 2 YEAR FOLLOW-UP SELF-CONTROLLED
STUDY ON MORPHOLOGICAL CHANGES IN THE MUSCULOSKELETAL APPARATUS AFTER CONSERVATIVE TREATMENT OF CONDYLAR HEAD FRACTURE Article Open access 13 May 2025 THE MAGNETIC RESONANCE IMAGING
EVALUATION OF CONDYLAR NEW BONE REMODELING AFTER YANG’S TMJ ARTHROSCOPIC SURGERY Article Open access 04 March 2021 THE INFLUENCE OF WISDOM TOOTH IMPACTION AND OCCLUSAL SUPPORT ON MANDIBULAR
ANGLE AND CONDYLE FRACTURES Article Open access 16 April 2021 INTRODUCTION Mandibular condyle is a fracture that frequently occurs in younger children. It is of special consequence because
the condyle is considered a primary growth centre of the jaw1,2. Intracapsular fractures are found predominantly amongst young children and are generally treated by closed treatment. To
date, many scholars generally hold the viewpoint that the displaced medial fragment could remodel into its original position even when the medial fragment was notably displaced, and the
shortening of the ramus height had been restored according to the capacity for remodelling3. However, other scholars denied this view and considered that the reduction of the fracture does
not generally occur under closed treatment4. However, evidence is insufficient. Our previous research found that the upright position of the fracture fragments of condylar neck or base
originates from the skeleton remodelling, rather than the anatomical reduction of the deviated condylar processes5. Therefore, this study aims to explore and impart understanding of bone
remodelling in children with intracapsular fractures treated conservatively. We hypothesised that the fracture fragment of the condyle determines the ramus height of the mandible. Present
study has found that the ramus height of the mandible is determined by the height of the fracture fragments (or medial process of condyle) in children with intracapsular condylar fractures
treated by conservative treatment. In addition, this study indicates that closed treatment cannot restore the fracture fragment in children with intracapsular condylar fractures. If the
height of the fracture fragments dropped remarkably, then open reduction and rigid internal fixation become more suitable. PATIENTS AND METHODS From March 2011 to February 2016, 22 patients
(less than 12 years) with intracapsular fractures treated conservatively were reviewed retrospectively and consecutively. The institutional review board of Wuhan University approved the
protocol, survey and consent forms (approval number: HGGC-146). The study was conducted in accordance with the Helsinki declaration and national regulation on study involving humans.
Informed consent was obtained from the legal guardian(s) of all children. Records of children (less than 12 years)6,7 who sustained intracapsular fractures and treated conservatively, were
retrieved consecutively for the period of March 2011 to February 2016. Data about age, gender, date of injury, dates of admission and discharge, mechanism of trauma, location and pattern of
fracture, other mandibular fracture, treatment methods and time of review were recorded and analysed. Image dates of pre- and post-treatment, including date of review, were also recorded.
Patients or files were excluded as study subjects based on the following: (1) incomplete information (especially the radiographic data), (2) lack of follow-up data (especially the
radiographic data) and (3) intracapsular condylar fractures treated surgically. The condylar head fractures (intracapsular fractures) were divided into three portions, namely, lateral third
(type A), central third (type B), medial third fractures (type C) and comminuted fracture of condylar head (type M), as proposed by He et al.8. Patients with type A/B/C fractures were
included in the present study, whereas type M fractures were excluded because the ramus height of the mandible decreased seriously during injury. Conservative treatment of intracapsular
condylar fractures was indicated in present cases, as follows: (1) children less than 12 years, (2) intracapsular condylar fracture was not treated surgically before and/or not treated
previously in other hospital, (3) new fracture less than 3 weeks. Conservative treatment included occlusal splint combined with maxillo-mandibular traction (achieved by self-drilling
cortical bone screws) for 4 weeks, patients were asked to eat fluid diet and do functional training (practice active mouth-opening exercises) in this period. After 4 weeks, the occlusal
splint and screws were removed. Based on the exclusion criteria, 22 patients have completed their follow-up and have shown bone remodelling process. STATISTICAL ANALYSES Descriptive analysis
was performed with the SPSS software (version 19.0; SPSS, Chicago, IL). The continuous variables were reported as mean ± SD. RESULTS In the five-year records retrieved during this study, 22
young patients were found to have sustained intracapsular condylar fractures. Amongst them, 14 were boys and eight were girls with a boy/girl ratio of 1.75:1; 15 children were unilateral
and seven were bilateral. Patients with intracapsular condylar fractures ranged from 2.4 to 11 years old, with a mean age of 6.68 ± 2.36 years. The shortest time of absorption in computed
tomography scan, observed in 31st day and the longest time in 415th day (average time of 112.68 ± 82.95 days). Fall-related accidents were the most common mechanism of injury (14 patients,
63.6%), followed by motor vehicle and motorcycle accidents (five patients, 22.7%). Table 1 shows the details of young patients with intracapsular condylar fractures treated by conservative
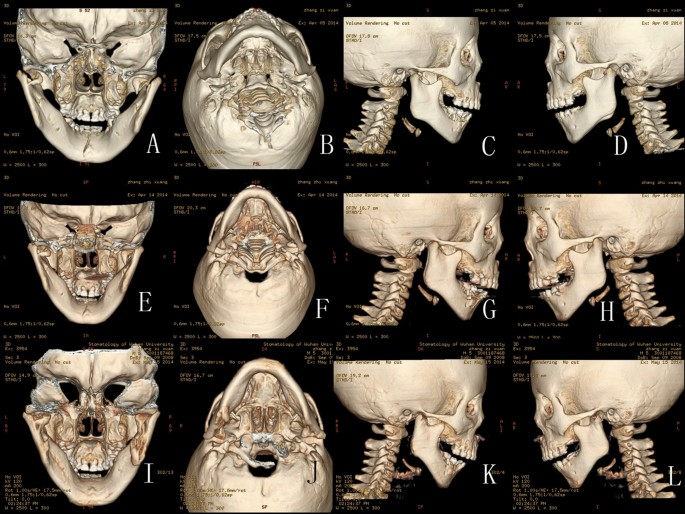
procedures. During their follow-up, all displaced condylar fragments fused with the ramus stump at the displaced position. Regardless of the type of conservative procedure, both treatments
cannot promote the spontaneous fracture reduction in patients with intracapsular condylar fractures. During follow-up, the absorption of the lateral process of the condyle after the closed
treatment was close to the ‘horizontal absorption’ until the height (or articular surface) of the lateral condylar process dropped and aligned to the articular surface of the medial process.
Sometimes, the simultaneous occurrence of the abduction of condylar head and the displacement of the medial process (fracture fragments) inferiorly lead to the mixed vertical and horizontal
absorption. No children patients presented ankylosis of temporomandibular joint during their follow-up. Figures 1, 2, 3, 4, 5 show the detailed bone remodelling. DISCUSSION Intracapsular
condylar fractures are found predominantly amongst young children and are generally treated by conservative treatment. To date, many scholars generally hold the viewpoint that the displaced
medial fragment could remodel into its original position even when the medial fragment was notably displaced, and the shortening of the ramus height had been restored according to the
remodelling capacity. This study found that the use of any conservative method to promote spontaneous fracture reduction in patients with intracapsular condylar fractures is impossible.
During follow-up, the absorption of the lateral process of the condyle after the conservative treatment was close to the ‘horizontal absorption’, until the height (or articular surface) of
the lateral condylar process dropped and aligned to the articular surface of the medial process. These findings have an important impact on clinical practice. This discovery reminds us that
the ramus height of the mandible is determined by the height of the fracture fragments (or medial process of condyle) in children with intracapsular condylar fractures treated by closed
treatment. If the height of the fracture fragments dropped remarkably, then open reduction and rigid internal fixation may be more suitable. Therefore, further researches are needed in the
future. After the occurrence of intracapsular condylar fractures, the continued traction of the lateral pterygoid muscle results in the anteromedial displacement of the fragment in condylar
head fractures9. A previous study10 revealed that immediately after injury, nearly all intracapsular condylar fractures showed anteromedial displacement of the disc and fractured condylar
fragment. Even at 3 months after injury, all patients continued to exhibit displacement of the disc and the condylar segments. In our previous study, we found that the upright position of
the extracapsular condylar fragments originates from the remodelling of the skeleton rather than the anatomical reduction of the deviated condylar processes5. This study observed that the
use of occlusal splint (or any other conservative methods) to promote the spontaneous fracture reduction in patients with intracapsular condylar fractures is impossible because the
horizontal traction force of the lateral pterygoid muscle cannot be eliminated under those circumstances. Ellis and Throckmorton4 do not use the term ‘closed reduction’, which they believe
is a misnomer, because reduction of the fracture dose not generally occur spontaneously. Nonetheless, the removable occlusal splint11,12 is widely used because it is easy to fabricate and
comfortable for children to wear; it helps re-establish normal occlusion and allows the mandible to maintain appropriate relationship with the maxilla. In addition, it allows early
mobilisation, eating and mandibular exercises and promote haematoma resolution and tissue recovery12. They12 even stated that wearing the occlusal splint followed by regular exercises
resulted in good mandibular function and condylar remodelling in children patients; no patient had TMJ symptoms and ankylosis. In the past, most previous studies claimed successful
remodelling once the condyle head was reconstructed into an arc (or oval) shape. Thorén13 found that incomplete remodelling with a flattened or irregular surface of the condylar head
associated with deformation of the condylar neck was frequently observed after condylar fracture in childhood. However, some authors had observed that the fractured fragments resorbed
completely but with acceptable condylar remodelling14. Other authors12 showed that in children with unilateral fractures, the condyles were incompletely remodelled with relatively short and
flattened condylar heads and flattened glenoid fossa compared with the contralateral normal condyles; most of their patients (children) showed slight difference in length between the
fractured and contralateral ramus. Some patients showed condylar deformity15 and altered mandibular growth16. However, they were usually only judged by visual observation. Previous studies
cannot easily provide direct evidence to answer whether or not condylar head resorption exists. This study presents the detailed process of condylar head resorption, but more studies are
needed in the future. The horizontal absorption of the lateral process of the condyle after the closed treatment is surprising. The absorption of the residual condylar head is different from
the resorption of the lateral condylar head because of the abduction of the condylar process17. Abduction leads to the ‘vertical absorption’ until condylar head located at the concentric
position of the glenoid fossa. In the present study, the absorption of the lateral process of the condyle after the closed treatment was close to the ‘horizontal absorption’, until the
height (or articular surface) of the lateral condylar process dropped and aligned to the articular surface of the medial process. Sometimes, the simultaneous occurrence of the abduction of
condylar head and the displacement of the medial process (fracture fragments) inferiorly lead to the mixed vertical and horizontal absorption. Surprisingly, this absorption only occurs in
children and is rarely found in adults in the above situation. He et al.18 indicated that the combination of an intracapsular fracture with concomitant widening of the mandible caused the
lateral pole of the condyle or the condylar stump to become displaced laterally or superolaterally in relation to the zygomatic arch, where it fused and formed the TMJ ankylosis. Chang et
al.3 found that three of the 23 children developed TMJ ankylosis due to ramus stumps displaced laterally and made contact with the root of the zygoma. In the present study, no TMJ ankylosis
was found. The important reason is that none of our patients’ condylar stump was displaced laterally or superolaterally to the zygomatic arch post-trauma or after intervention. Clinically
over the past decades, we rarely found the occurrence of TMJ ankylosis in children with intracapsular condylar fractures in our department. Zhao et al.12 also found no patient (40 children
with condylar fractures, most children patients suffered high-neck fractures and intracapsular fractures) had TMJ symptoms and ankylosis. Therefore, we also speculate that the presence of
articular cartilage in children prevented them from developing TMJ ankylosis, in spite of the disc displaced anteromedially; whereas in adult, articular cartilage of condyle is generally
degenerated. However in present study, we didn’t use Magnetic Resonance Imaging (MRI). Therefore, we can’t assess disc displacement. Some limitations could be found in this study. First, it
is a retrospective study with small sample size. The small size reduced the power but provided the discovery unreported previously. Second, the cases were only obtained from our own hospital
(maxillofacial trauma service), some paediatric patients could be brought for care in other children’s hospital, and multicentre and more sample studies are necessary in the future.
However, our department was amongst the largest centres for patients with facial trauma in central China, and the children patients were treated consecutively with nearly no omission. Thus,
we consider our findings similar to those other large maxillofacial urban units in China. In conclusion, in children with intracapsular condylar fractures, the fracture fragment of the
condyle determines the ramus height of the mandible. Closed treatment cannot restore the fracture fragment. If the height of the fracture fragments dropped remarkably, then open reduction
and rigid internal fixation become more suitable. REFERENCES * Smartt, J. M. Jr., Low, D. W. & Bartlett, S. P. The pediatric mandible: II. Management of traumatic injury or fracture.
_Plast. Reconstr. Surg._ 116(2), 28e–41e. https://doi.org/10.1097/01.prs.0000173445.10908.f8 (2005). Article PubMed Google Scholar * Lopez, J. _et al._ Noninvasive management of pediatric
isolated, condylar fractures: Less is more?. _Plast. Reconstr. Surg._ 147(2), 443–452. https://doi.org/10.1097/PRS.0000000000007527 (2021). Article CAS PubMed Google Scholar * Chang, S.
_et al._ How does the remodeling capacity of children affect the morphologic changes of fractured mandibular condylar processes after conservative treatment?. _J. Oral Maxillofac. Surg._
76(6), 1279.e1271-1279.e1277. https://doi.org/10.1016/j.joms.2018.01.029 (2018). Article Google Scholar * Ellis, E. & Throckmorton, G. S. Treatment of mandibular condylar process
fractures: Biological considerations. _J. Oral Maxillofac. Surg._ 63(1), 115–134. https://doi.org/10.1016/j.joms.2004.02.019 (2005). Article PubMed Google Scholar * Zhou, H. H., Lv, K.,
Yang, R. T., Li, Z. & Li, Z. B. Extracapsular condylar fractures treated conservatively in children: Mechanism of bone remodelling. _J. Craniofac. Surg._ 32(4), 1440–1444.
https://doi.org/10.1097/SCS.0000000000007237 (2021). Article PubMed Google Scholar * Zhou, H. H., Ongodia, D., Liu, Q., Yang, R. T. & Li, Z. B. Incidence and pattern of maxillofacial
fractures in children and adolescents: A 10 years retrospective cohort study. _Int. J. Pediatr. Otorhinolaryngol._ 77(4), 494–498. https://doi.org/10.1016/j.ijporl.2012.12.017 (2013).
Article PubMed Google Scholar * Yuan, Y. & Chai, Y. Regulatory mechanisms of jaw bone and tooth development. _Curr. Top. Dev. Biol._ 2019(133), 91–118.
https://doi.org/10.1016/bs.ctdb.2018.12.013 (2019). Article CAS Google Scholar * He, D., Yang, C., Chen, M., Jiang, B. & Wang, B. Intracapsular condylar fracture of the mandible: Our
classification and open treatment experience. _J. Oral Maxillofac. Surg._ 67(8), 1672–1679. https://doi.org/10.1016/j.joms.2009.02.012 (2009). Article PubMed Google Scholar * Tang, Y.,
Wang, X., Zhu, Y., Sun, H. & Zhu, M. A Comparative evaluation of CBCT outcomes of two closed treatment methods in intracapsular condylar fractures. _Oral Surg. Oral Med. Oral Pathol.
Oral Radiol._ 123(5), e141–e147. https://doi.org/10.1016/j.oooo.2016.11.019 (2017). Article PubMed Google Scholar * Yang, X. _et al._ Does soft tissue injury affect intracapsular condylar
fracture healing?. _J. Oral Maxillofac. Surg._ 73(11), 2169–2180. https://doi.org/10.1016/j.joms.2015.05.030 (2015). Article PubMed Google Scholar * Wu, Y. _et al._ Management of
paediatric mandibular condylar fractures with screw-based semi-rigid intermaxillary fixation. _Int. J. Oral Maxillofac. Surg._ 41(1), 55–60. https://doi.org/10.1016/j.ijom.2011.09.006
(2012). Article CAS PubMed Google Scholar * Zhao, Y. M., Yang, J., Bai, R. C., Ge, L. H. & Zhang, Y. A retrospective study of using removable occlusal splint in the treatment of
condylar fracture in children. _J. Cranio Maxillofac. Surg._ 42(7), 1078–1082. https://doi.org/10.1016/j.jcms.2012.07.010 (2014). Article Google Scholar * Thoren, H., Iizuka, T.,
Hallikainen, D. & Lindqvist, C. Radiologic changes of the temporomandibular joint after condylar fractures in childhood. _Oral Surg. Oral Med. Oral Pathol. Oral Radiol Endod._ 86(6),
738–745. https://doi.org/10.1016/S1079-2104(98)90214-1 (1998). Article CAS PubMed Google Scholar * Zou, Z. J. _et al._ Remodelling of the temporomandibular joint after conservative
treatment of condylar fractures. _Dentomaxillofac. Radiol._ 16(2), 91–98. https://doi.org/10.1259/dmfr.1987.0013 (1987). Article CAS PubMed Google Scholar * Strobl, H., Emshoff, R. &
Rothler, G. Conservative treatment of unilateral condylar fractures in children: A long-term clinical and radiologic follow-up of 55 patients. _Int. J. Oral Maxillofac. Surg._ 28(2), 95–98
(1999). Article CAS PubMed Google Scholar * Hovinga, J., Boering, G. & Stegenga, B. Long-term results of nonsurgical management of condylar fractures in children. _Int. J. Oral
Maxillofac. Surg._ 28(6), 429–440. https://doi.org/10.1034/j.1399-0020.1999.280606.x (1999). Article CAS PubMed Google Scholar * Zhou, H. H. _et al._ Abduction of the condyle head leads
to condylar resorption: A radiologic study in children with intracapsular fractures. _Int. J. Pediatr. Otorhinolaryngol._ 123, 168–174. https://doi.org/10.1016/j.ijporl.2019.05.013 (2019).
Article PubMed Google Scholar * He, D., Ellis, E. 3rd. & Zhang, Y. Etiology of temporomandibular joint ankylosis secondary to condylar fractures: The role of concomitant mandibular
fractures. _J. Oral Maxillofac. Surg._ 66(1), 77–84. https://doi.org/10.1016/j.joms.2007.08.013 (2008). Article PubMed Google Scholar Download references AUTHOR INFORMATION AUTHORS AND
AFFILIATIONS * The State Key Laboratory Breeding Base of Basic Science of Stomatology (Hubei-MOST) & Key Laboratory of Oral Biomedicine Ministry of Education, School & Hospital of
Stomatology, Wuhan University, Wuhan, People’s Republic of China Rui-cong Yang, Meng-juan Cui, Hai-Hua Zhou, Kun Lv, Rong-Tao Yang, Zhi Li & Zu-Bing Li * Department of Oral and
Maxillofacial Surgery, College and Hospital of Stomatology, Wuhan University, 237 Luoyu Road, Wuhan, 430079, Hubei, People’s Republic of China Hai-Hua Zhou, Kun Lv, Rong-Tao Yang, Zhi Li
& Zu-Bing Li Authors * Rui-cong Yang View author publications You can also search for this author inPubMed Google Scholar * Meng-juan Cui View author publications You can also search for
this author inPubMed Google Scholar * Hai-Hua Zhou View author publications You can also search for this author inPubMed Google Scholar * Kun Lv View author publications You can also search
for this author inPubMed Google Scholar * Rong-Tao Yang View author publications You can also search for this author inPubMed Google Scholar * Zhi Li View author publications You can also
search for this author inPubMed Google Scholar * Zu-Bing Li View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS Conceived and designed the
experiments: R.C.Y., M.J.C., H.H.Z. Analysed the data: R.C.Y., M.J.C., H.H.Z. Wrote the paper: R.C.Y., H.H.Z. Substantial contribution to acquisition of data: H.H.Z. Critically revised
article for important intellectual content: R.C.Y., M.J.C., H.H.Z., K.L., R.T.Y., Z.L., Z.B.L. Critically reviewed the manuscript: H.H.Z. Approved the final version of the manuscript: H.H.Z.
CORRESPONDING AUTHOR Correspondence to Hai-Hua Zhou. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no competing interests. ADDITIONAL INFORMATION PUBLISHER'S NOTE
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. RIGHTS AND PERMISSIONS OPEN ACCESS This article is licensed under a
Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit
to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are
included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons
licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of
this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Yang, Rc., Cui, Mj., Zhou, HH. _et al._ Fracture fragment of
the condyle determines the ramus height of the mandible in children with intracapsular condylar fractures treated conservatively. _Sci Rep_ 12, 19924 (2022).
https://doi.org/10.1038/s41598-022-24463-4 Download citation * Received: 21 October 2021 * Accepted: 15 November 2022 * Published: 19 November 2022 * DOI:
https://doi.org/10.1038/s41598-022-24463-4 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link Sorry, a shareable link is not
currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative
Trending News
Oops! That page can't be foundOops! That page can't be found It seems we can't find what you're looking for.Latest from HITC More latest from HITC...
People only just realising 'fascinating' reason uk cities have specific namesHAVE YOU EVER WONDERED WHY MANY PLACES AROUND THE UK HAVE SIMILAR NAME ENDINGS? THEY ARE NOT JUST RANDOM, AND EACH HAS A...
information - 1jour1actu.comRECEVEZ L'ACTU DU JOUR ! Pour recevoir tous les jours les articles et vidéos d'1jour1actu, merci de renseignez...
7 best shoes under ₹500 price range that you can buy online - scoopwhoop‘Good shoes take you good places’. Whether or not you believe in this phrase, shoes still remain an important part of ou...
Pressure for environmental disclosure increasesCompanies urged to measure their carbon costs. Access through your institution Buy or subscribe This is a preview of sub...
Latests News
Fracture fragment of the condyle determines the ramus height of the mandible in children with intracapsular condylar fractures treated conservativelyABSTRACT This study aimed to explore and impart understanding of bone remodelling in children with intracapsular fractur...
RBI-MONEY-MARKET-OPERATIONMoney Market Operations as on FEB 01, 2016 (Amount in Rupees billion, Rate in per cent). MONEY MARKETS @ Volume Wtd.Avg....
Travis kelce footing hefty super bowl suite bill for his and taylor swift’s familyTravis Kelce is taking care of his main squeeze Taylor Swift and their families at Super Bowl 2024. After the Chiefs’ st...
Page Not Found很抱歉,你所访问的页面已不存在了。 如有疑问,请电邮[email protected] 你仍然可选择浏览首页或以下栏目内容 : 新闻 生活 娱乐 财经 体育 视频 播客 新报业媒体有限公司版权所有(公司登记号:202120748H)...
Tackling the climate change challenge the ‘green’ wayThe Center for Environment Education (CEE) and the Earth Charter Initiative is jointly hosting an international conferen...