Results of the german migraine patient survey on medical care and prophylactic treatment experience (episcope)
Results of the german migraine patient survey on medical care and prophylactic treatment experience (episcope)"
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT Migraine affects about 12% of the worldwide population causing substantial personal and societal burden. Yet, migraine remains underdiagnosed and untreated. EPISCOPE was a web-based
survey among a German migraine patient cohort to characterize the medical care and prophylactic treatment status aiming to identify unmet needs. Potential migraine patients were identified
via an ID Migraine screener. Their socioeconomic background, medical care experience, acute medication use, as well as use and experience of migraine prophylaxis was assessed by a
questionnaire. Data of 29,011 participants was collected. 21,504 participants were identified as migraine patients. Patients with a higher number of monthly migraine days experienced better
medical care. However, even among chronic migraine patients, 54% were not consulting a physician, 30% did not feel well-informed about medication overuse and 48% had never tried prophylactic
migraine treatment. Among patients receiving prophylactic migraine treatment, up to 33% were not satisfied with their prophylaxis due to insufficient efficacy. Taken together, EPISCOPE
describes the largest German migraine patient cohort so far. The survey provides detailed and valuable insight into the current medical care and prophylactic treatment situation in a highly
developed European country and identifies reasons why the medical care of migraine patients is still insufficient. SIMILAR CONTENT BEING VIEWED BY OTHERS LOW ADHERENCE TO THE GUIDELINE FOR
THE ACUTE TREATMENT OF MIGRAINE Article Open access 19 May 2022 DIAGNOSIS AND MANAGEMENT OF MIGRAINE IN TEN STEPS Article Open access 18 June 2021 MEDICATION ADHERENCE IN PATIENTS WITH
CLUSTER HEADACHE AND MIGRAINE: AN ONLINE SURVEY Article Open access 20 March 2023 INTRODUCTION Migraine is a common headache disorder that affects numerous important areas of life, including
physical and psychological health, career and interpersonal dynamics1. According to the Global Burden of Disease Report 2016 (GBD 2016) it ranks as the world’s second leading cause of
healthy life lost to disability (YLD). Therefore, the socioeconomic impact of migraine is enormous. Nevertheless, migraine is commonly underdiagnosed and undertreated not only in poorer
countries but also in wealthy nations such as Europe and North America2,3,4. In Germany, only 8–11% of migraine patients used triptans and less than 3% of patients with ≥ 5 monthly migraine
days (MMD) received preventative treatment2,5. We sought to verify this and to identify in more detail the reasons for underdiagnosis and undertreatment of migraine patients in Germany by
analysing data from the EPISCOPE study. EPISCOPE was an online survey that gathered data from a large cohort of self-identified migraine patients in Germany. As the aim of this study was to
analyse the medical care of migraine patients, individuals who did not consider themselves to have migraine were excluded from the analysis. The survey included diagnostic inquiry regarding
migraine and further exploration regarding the patient journey from disease onset to diagnosis and utilisation of medical services, medication and non-pharmacological therapies for migraine.
Here, we present data on the current status of diagnosis and treatment of migraine patients in Germany, including consultations and migraine-specific acute and preventative medications, as
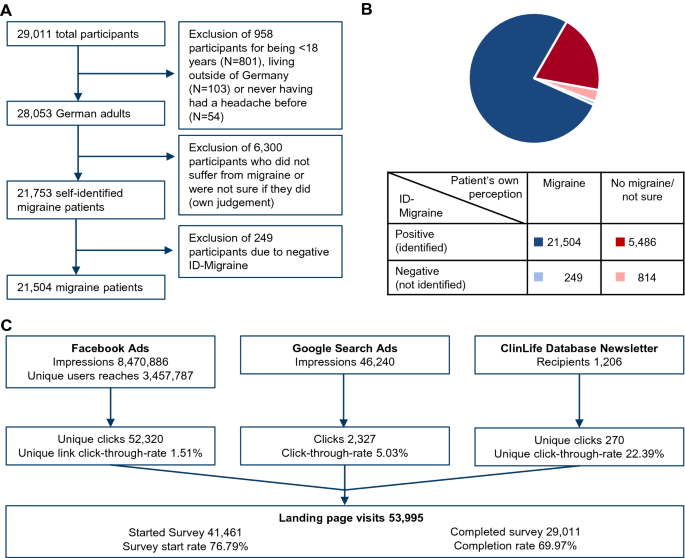
well as the reasons for underdiagnosis and undertreatment of migraine in Germany. RESULTS DEMOGRAPHIC DATA From 53,995 landing page visits, 41,461 individuals started the survey, and 29,011
completed it (completion rate of 69.97%; Fig. 1C). Of 29,011 participants, 958 were excluded because they were younger than 18 years (N = 801), lived outside of Germany (N = 103) or had
never had a prior headache (N = 54) (Fig. 1A). The remaining 28,053 participants underwent an ID Migraine screener, which consisted of three questions to validate whether the participant is
indeed suffering from migraine (Supplementary Table S1). If two out of three questions were affirmed, a participant was identified as a migraine patient. According to their own judgement,
78% (N = 21,753) of all German participants considered themselves as migraine patients while 22% (N = 6300) stated they did not suffer from migraine or were unsure if they did (Fig. 1B). As
we wanted to analyse the medical care of migraine patients, we excluded all participants from answering further questions who did not consider themselves as migraine patients. Amongst all
participants who stated that they suffered from migraine, the subsequent well established ID Migraine screener identified 99% (N = 21,504) as potential migraine patients, resulting in the
exclusion of an additional 249 participants from the study. The ID Migraine screener additionally revealed that of the 6,300 participants who stated that they did not suffer from migraine or
were unsure if they did, the vast majority (87%, N = 5486) also suffered from migraine. If not specifically indicated, only patients living in Germany, initially stated that they were
suffering from migraine and had a positive ID Migraine screener result (N = 21,504) were considered for the following analyses. Most migraine patients, 85.5% (N = 18,390), were female, while
14.3% (N = 3077) male and 0.2% (N = 37) were diverse. The mean age of migraine patients were 29.2 ± 10.01 years and the majority was employed (71.4%, N = 15,345), while 1.7% (N = 356) had
limited employment due to migraine, 0.8% (N = 161) were not able to work due to migraine, and 0.4% retired early due to migraine (N = 89) (Table 1). CLINICAL DETAILS The mean time since
migraine onset was 13.4 ± 9.9 years, and the mean monthly days (MMDs) in the three months before the survey was 5.7 ± 5.4 (Table 1). 46.1% (N = 9920) of patients reported < 4 MMD, 29.3%
(N = 6297) 4–7 MMD, 15.4% (N = 3313) 8–14 days and 9.2% (N = 1974) reported ≥ 15 MMD. MEDICAL CARE Of all identified migraine patients in this survey, 74% (N = 15,994) were diagnosed by a
physician (Fig. 2A). 54% (N = 8558) received the diagnosis within two years after onset of their migraine, 21% (N = 3379) of patients were diagnosed 2–5 years after migraine onset, and 15%
(N = 2455) of patients received the diagnosis more than 5 years after symptom onset. Most diagnoses were made by neurologists (52%, N = 8256), followed by general practitioners (39%, N =
6198) and pain specialists (3%, N = 513) (Supplementary Figure S1A). The proportion of patients diagnosed within 2 years was highest among general practitioners, followed by internists and
gynaecologists; neurologists, pain specialists and orthopaedists saw a higher proportion of patients diagnosed after more than 5 years (Supplementary Figure S1B). Although 74% of identified
migraine patients were diagnosed by a physician, only 26% (N = 5629) were receiving any kind of treatment at the time of the survey. Even among patients with ≥ 15 MMD only 43% (N = 842)
visited a doctor (Supplementary Figure S1C). Migraine patients thereby mostly sought help from general practitioners and neurologists, and the percentage of patients seeing neurologists
compared to general practitioners increased with the amount of MMD (Fig. 2B). As main reasons against seeking medical advice, most patients stated that they had their migraine under control
with or without usage of acute medication (Fig. 2C). While 51% (N = 4137) of patients with < 4 MMD managed their migraine with acute medication, only 32% (N = 357) of patients with ≥ 15
MMD were able to do so. Similarly, while 17% (N = 1420) of patients with < 4 MMD had their migraine under control even without acute medication, this applied to only 7% (N = 84) of
patients with ≥ 15 MMD. Furthermore, 14% (N = 2145) of patients across all MMD groups considered the waiting time for a specialist’s appointment too long and 12% (N = 1934), especially
younger patients, were not sure which specialist to consult (Supplementary Figure S1D, right panel). ACUTE MEDICATION More than 90% of all identified migraine patients used acute medication
at least once per month with a similar number of acute medication days across gender and age (Supplementary Figure S2). The mean days of acute medication use per patient increased with
rising number of MMD (Fig. 3A). When patients were asked about their knowledge of medication overuse, 69% (N = 14,758) stated “I know when medication overuse can occur and its risks”, while
19% (N = 4137) indicated “I have heard about medication overuse but I don’t know much about it” and 12% (N = 2609) declared “I know (almost) nothing about medication overuse” (Fig. 3B).
Patients who had already tried multiple preventative treatments felt better informed than those who had never tried any prophylaxis (Fig. 3B). Similarly, patients with more MMDs had better
knowledge about medication overuse than patients with fewer MMDs (Supplementary Figure S2D). PROPHYLAXIS The number of migraine patients who had previously tried at least one preventative
treatment increased with the number of MMD (filled blue stacks, Fig. 4A). However, even among patients with ≥ 15 MMD, half (51%, N = 997) had never tried prophylactic migraine treatment.
Patients with more MMDs have cycled through a higher number of different prophylaxes than patients with fewer MMD. The main reasons for discontinuation were thereby the occurrence of side
effects, ranging from 48% (N = 468) among patients with less than four MMD to 54% (N = 316) in the group with greater than or equal to 15 MMD, and lack of efficacy, which ranged from 36% (N
= 346, 4 < MMD) to 54% (N = 312, ≥ 15 MMD) (Fig. 4B). In addition, among patients who were still on prophylactic treatment at the time of the survey, between 10% (patients with < 4
MMD) and 30% (patients with ≥ 15 MMD) were not satisfied with their current prophylaxis due to insufficient efficacy (Fig. 4C). When asked about their three most important demands on a new
prophylactic treatment, most patients named good tolerability (75%, N = 16,043), fast onset of effect (68%, N = 14,657) and good efficacy (60%, N = 12,963) (Fig. 4D). DRUG-FREE PROPHYLACTIC
TREATMENTS 47% (N = 10,068) of all identified migraine patients had previously tried drug-free prophylactic treatment with an increasing incidence depending on the number of MMD (Fig. 5A).
At the time of the survey, most patients were carrying out stamina training (N = 3499; 16% of all identified migraine patients), followed by relaxation training (N = 2652; 12% of all
identified migraine patients) (Fig. 5B). In general, more women than men have tested drug-free prophylactic treatments, and the number of patients that have tried drug-free prophylactic
treatments was higher among patients who have already discontinued at least one prophylactic drug therapy (Supplementary Figure S3). DISCUSSION EPISCOPE is the largest survey among migraine
patients in Germany to date and provides insights into clinical aspects and reasons for insufficient use of medical care by migraine patients in Germany. EPISCOPE was performed as an online
survey, advertised specifically among people who were identified as potential migraine patients via a Facebook algorithm. The advertisements were designed to appeal to people’s interest
towards migraine or their willingness to help improve awareness of migraine disease, and thus resulted in an interest-guided study population. As seen before in other online studies6, the
population questioned was younger than migraine populations seen in clinical trials7,8,9 or population based studies2. However, Lipton et al. previously showed that the age difference
between participants of online and mail surveys did not have a differential effect on the results concerning disease burden and medical need6. EPISCOPE invited all migraine patients to
participate independent of their MMDs and previous use of migraine-specific prophylaxis. EPISCOPE therefore expands the findings of other studies, which were restricted to patients with
multiple treatment failures, high medical need, or had more than four MMDs10. This study analysed different aspects of a patient’s journey. The first step of this journey is awareness of the
disease. The study revealed that even in a population presumably biased by interest towards migraine there is still a substantial percentage of people who may not be aware of their disease.
These results are in line with previous studies in Germany11 and France12. Part of this problem is probably related to patients disbelieving or even stigma: a social construct that serves
to promote inequity for patients afflicted with various disease states13. Stigma carries negative social consequences but also impacts medical care of those who are stigmatised. Stigmatised
patients are less likely to seek care. Indeed, the EUROLIGHT study clearly demonstrated that only a small part of people with migraine in Europe received adequate medical care 2. An earlier
study in Turkish immigrants in Germany has shown that social disparities influence access to medical care, too14. Thus, poor awareness of people with migraine is one of the factors why they
do not seek medical care. Deficiencies in the available system of medical care might be another obstacle. Migraine care should be initiated and maintained in primary care for most affected
individuals. In Europe, primary care can meet the needs of the majority of individuals who consult their primary care physician because of headaches15 since most of these individuals suffer
from either migraine or tension-type headache. General practitioners require basic skills to diagnose migraine, exclude secondary causes, and initiate treatment16,17. Patients mostly with
treatment-resistant or refractory migraine, rare headache disorders or medication overuse headache may require referral to specialist care. Benefits from specialist care are likely
attributed to higher levels of expertise and availability of a multidisciplinary team. However, structured specialist services are scarce even in developed countries, e.g. Germany15. In
addition, existing specialist services are often limited by long delays from the point of referral to consultation which is only to the detriment of the affected patients. In our study, the
long waiting time was one of the most frequent reasons for not seeing a doctor, especially a specialist. Besides that, young patients in particular were uncertain about which health care
professional to consult, which hints at a lack of awareness and further need for education of the German migraine population. Nevertheless, the proportion of patients who have received a
migraine diagnosis by a doctor and the proportion of patients who consulted a doctor in our study were higher than the average reported in the European Community2, which was probably due to
the bias in our patient cohort discussed above. It is also not surprising that migraine burden, e.g. high frequency of migraine attacks, was the major driving force for seeking medical
consultation. Similarly, severely affected patients were better informed and more willing to take acute and preventative medication. Our study demonstrated once again that even in a European
country like Germany, with a well-developed system of medical care, the quality of treatment received by surveyed patients with headache was poor. More than 90% of patients used medications
to treat migraine attacks but only a small proportion used preventative medication continuously. The German guidelines recommend starting preventative medication in patients with more than
4 MMD, especially in those with more than 8 MMD18. In our study, even in the group of patients with greater than or equal to 15 MMD half of them have never tried preventive treatment.
Preventive medication was more frequently given by specialists than general practitioners. This finding is not specific for Germany but in line with previous reports2 that show broad
differences in the education of physicians, as demonstrated by large discrepancies between general practitioners and neurologists concerning their prescription rate of preventive migraine
treatment. In addition, among patients who have decided to try preventative drug therapy the adherence to this treatment was very low. These results concur with what has been described by
Hepp et al.19 and illustrate again that many patients are not satisfied with the existing standard medications. The main reasons for discontinuation were dissatisfaction with the efficacy of
the preventative treatment or side effects, which reinforces the need for new efficient prophylactic treatments with fewer side effects and an improved efficacy. It has to be kept in mind
that EPISCOPE was conducted only a few months after the first representative of a new class of migraine prophylaxis, the calcitonin gene-related peptide (CGRP) pathway targeting monoclonal
antibody erenumab, was available in Germany and we therefore assume that the vast majority had not tried this new drug at the time of the survey. It will therefore be very interesting to see
if this new class of prophylaxis will be able to better satisfy the patients’ needs with regard to safety and efficacy which is already being investigated in a recently closed trial
(NCT03828539). Besides the preventive care there is also need to further investigate the use of acute medication (RX, OTC), potential barriers of their use, the perceived effectiveness and
their potential as another approach to improve migraine care. In the EPISCOPE survey the consulted migraine patients receive insufficient medical care; however, there are some limitations of
the study that should be considered. First, it has to be kept in mind that the recruitment via targeted online advertisement resulted in an interest-guided study population and thus the
population questioned was younger compared to other online studies6. Therefore, older migraine cases may be underrepresented in this study. Furthermore, this study does not provide any
information on the medical care of people unaware of their own suffering from migraine or reasons for the lack of their awareness. Second, this study used the three item ID migraine
screener, which is a well-established and reliable screening tool for migraine20. However, it must be remembered that this does not equal a validated migraine diagnosis as per ICHD-3
criteria. Around 25% of the participants who stated that they were suffering from migraine, did not have a medical diagnosis or were not sure whether a migraine had been diagnosed
previously. Although these participants had a positive ID Migraine screener result, this population could include a proportion of patients that does not suffer from migraine but another
headache disorder. Third, EPISCOPE did not capture the disease burden of migraine patients beyond disease duration and number of MMD. Further studies will be necessary to assess the
correlation of medical care and quality of life parameters and to investigate how new migraine prophylaxes will affect disease burden. Fourth, the analysis eliminated individuals from the
sample who met ID-Migraine symptom criteria for migraine but who did not consider themselves to have migraine. Therefore, identification of reasons for underdiagnosis and undertreatment are
limited to those who believe they have migraine, and which is confirmed by the ID Migraine screener. Furthermore, as the migraine days are not confirmed by a symptom diary, the number of
migraine days may be overestimated, and the number of total headache days may be underestimated. Fifth, there may be a response and recall bias in a highly stigmatized condition as migraine.
EPISCOPE is the largest survey that has been conducted among the whole migraine patient population in Germany so far. Although Germany is a rich country with a well-developed medical care
system, the survey demonstrates insufficient medical care for the consulted migraine patients. Here, we identified three major reasons for this situation that need to be addressed in order
to improve the medical care situation of these migraine patients. First, lack of patient education, which affects awareness of the disease and consultation of medical health care
professionals. Second, limited access to specialist care including long waiting times which deters migraine patients from consultation and consequently prevents successful treatment of more
severely affected migraine patients. Lastly, the limited tolerability and efficacy of oral non-specific preventive therapies, which are currently the standard of care therapy in Germany, may
hinder migraine patients from trying a prophylactic therapy and those who do try may have a low treatment adherence due to the aforementioned limitations. Thus, we need earlier access to
targeted preventive therapies with a better tolerability such as antibodies targeting the CGRP pathway. METHODS The EPISCOPE survey was performed from January to March 2019. We approached
people in Germany suffering from migraine through a targeted media outreach campaign. The following advertising channels were used for the outreach campaign: social media advertising
(Facebook/Instagram), newsletter and search engine advertising. As EPISCOPE was an anonymous online survey and anonymous surveys do not require ethical approval according to German law. This
survey was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. The survey was rolled out by Clariness GmbH and was compliant with ethics guidelines.
Patients were informed about data storage, processing, and publication, and their informed consent was obtained. Before survey start, respondents had to confirm the informed consent on the
landing page of the survey. The informed consent explained the intent of the survey. It also described how much time the survey will probably take and that the survey is anonymous, and the
answers cannot be linked to the participants. The survey software is hosted on the fully secured server environment of Clariness GmbH in Germany which guarantees full compliance with all
legal requirements for the protection of the survey answers. The survey questions and response options were developed together by Clariness GmbH and the authors. First, a text document was
created in Word, in which all questions and answer options were listed. For each question there was also the information in which question format the question should be asked (single choice,
multiple choice, etc.). The document also described the conditions under which a question should be asked. This document was proofread and confirmed by the authors before being entered into
the survey software. A Patient Insights Manager set up the developed questionnaire. Before the survey was released, a quality check was performed. A second Patients Insights Manager checked
whether the settings were correct, and the questions were set up according to the document. Using a test link the authors performed a final test, followed by survey activation. Survey
pre-testing with a panel of migraine patients was not done. Survey respondents didn’t receive any incentive for their participation. To avoid multiple entries of the same respondent, a
cookie was placed in the internet browser of the participant after completion. When the respondent tried to start the survey again with the same internet browser, an error message was shown.
Since fully anonymous, open surveys can’t completely prevent multiple entries. Only fully completed questionnaires were used as data basis for the survey reporting. Almost all questions
displayed to the participants were made mandatory. So, it was technically not possible to continue the survey without providing an answer. Only exceptions on purpose: Q06 and Q07 (questions
about region and zip code). We have targeted users on Facebook/Instagram who are interested in migraine topics (e.g. “Prevention of migraines”, “Migraine News”). Participants’ attention was
attracted by different ad formats with a heading that was always connected to the catchphrase “Migraine”. Advertisement wording varied in order to reach a broad patient population: “Your
opinion is important for us”, “Your experiences are important”, “You are invited to participate in a migraine survey”, “You can help us to understand patients with migraine better” or “New
migraine survey is online”. To better control the demographic aspect, we have segmented the interest targeting by gender in two ad groups (female/male). After people who were interested
clicked on the advertisement, they were redirected to the landing page, where they were informed about the purpose of the survey and aspects of data protection. People who wanted to
participate in the survey could do so by clicking on the call-to-action button (“Start Survey”). To support the Facebook algorithm's purpose of showing our ads to users who are more
likely to complete the survey, the Facebook conversion pixel was implemented on our website. The newsletter was addressed to persons subscribed to the ClinLife “migraine” newsletter
(Opt-in). The survey comprised five domains and 36 questions, which were designed to obtain information about every step of the patient journey (Supplementary Table S2). The first domain
covered general baseline characteristics of all participants such as sex, age, and occupation. The second domain collected information on clinical details, including onset and prevalence of
their migraine and the ID Migraine screener (for ID Migraine questions see Supplementary Table S1) in order to identify those participants who did indeed suffer from migraine. The ID
Migraine screener is a brief, self-administered questionnaire for patients with headache complaints asking for disability, nausea and sensitivity to light (photophobia) (German version,
sensitivity of 99% and a specificity of 68%)20,21. In the next domain, participants were asked about the medical care they had, starting from questions about their diagnosis to their current
treatment situation. The fourth domain covered the topic of acute medication, including frequency of migraine-specific medication usage and patient education with regard to medication
overuse. In the last domain, the usage and patient view on prophylactic treatment was assessed, covering both drug and drug-free prophylactic treatments. Participants who were older than 18
years, lived in Germany and suffered from migraine confirmed by diagnostic questions of the survey (inclusion criteria) were entered for final analysis. ANALYSIS AND STATISTICS Participants
who stated that they did not suffer from migraine or were unsure if they did were excluded from answering the remaining questions—even if some of them were indeed identified as migraine
patients by the ID Migraine screener—as they did not consider themselves as migraine patients and therefore most likely never followed up on their disease. Participants were grouped based on
the headache frequency in the three months before the survey (monthly migraine days, MMD) in the four groups: low-frequency (< 4 MMD), medium-frequency (4–7 MMD), and high-frequency
episodic migraine (8–14 MMD), and chronic migraine (≥ 15 MMD), based on the age (18–25, 26–35, 36–45, 46–55, 56 + years) or based on the number of prophylactic treatments that they have
tried and discontinued (none tried, still on first prophylaxis, 2/3/4/ ≥ 5 discontinued). The analysis of the monthly migraine days of the survey participants is based on question Q08 (“How
often have you on average suffered from migraine within the last 3 months?”). Categorical variables were summarised as proportions (%) and frequencies (N), and continuous variables as means
± standard deviation (SD). The data was analysed using Tableau Reader. The analysis is purely descriptive, no statistical comparisons were performed. Figures were generated using Microsoft
PowerPoint. CONSENT TO PARTICIPATE Patients were informed about data storage, processing, and publication and their informed consent was obtained. Consent to publish is not applicable for
this survey. DATA AVAILABILITY The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request. REFERENCES * Buse, D. C. _et
al._ Life with migraine: Effects on relationships, career, and finances from the chronic migraine epidemiology and outcomes (CaMEO) study. _Headache_ 59, 1286–1299.
https://doi.org/10.1111/head.13613 (2019). Article PubMed PubMed Central Google Scholar * Katsarava, Z., Mania, M., Lampl, C., Herberhold, J. & Steiner, T. J. Poor medical care for
people with migraine in Europe—Evidence from the Eurolight study. _J. Headache Pain_ 19, 10. https://doi.org/10.1186/s10194-018-0839-1 (2018). Article PubMed PubMed Central Google Scholar
* Katsarava, Z., Buse, D. C., Manack, A. N. & Lipton, R. B. Defining the differences between episodic migraine and chronic migraine. _Curr. Pain Headache Rep._ 16, 86–92.
https://doi.org/10.1007/s11916-011-0233-z (2012). Article PubMed Google Scholar * WHO & Burden, L. T. _Atlas of headache disorders and resources in the world 2011._ (2011). * Yoon, M.
S. _et al._ Prevalence of primary headaches in Germany: results of the German Headache Consortium Study. _J. Headache Pain_ 13, 215–223. https://doi.org/10.1007/s10194-012-0425-x (2012).
Article PubMed PubMed Central Google Scholar * Lipton, R. B., Manack Adams, A., Buse, D. C., Fanning, K. M. & Reed, M. L. A comparison of the chronic migraine epidemiology and
outcomes (CaMEO) study and American Migraine Prevalence and Prevention (AMPP) study: Demographics and headache-related disability. _Headache_ 56, 1280–1289.
https://doi.org/10.1111/head.12878 (2016). Article PubMed PubMed Central Google Scholar * Reuter, U. _et al._ Efficacy and tolerability of erenumab in patients with episodic migraine in
whom two-to-four previous preventive treatments were unsuccessful: A randomised, double-blind, placebo-controlled, phase 3b study. _Lancet_ 392, 2280–2287.
https://doi.org/10.1016/S0140-6736(18)32534-0 (2018). Article CAS PubMed Google Scholar * Goadsby, P. J. _et al._ A controlled trial of erenumab for episodic migraine. _N. Engl. J. Med._
377, 2123–2132. https://doi.org/10.1056/NEJMoa1705848 (2017). Article CAS PubMed Google Scholar * Dodick, D. W. _et al._ ARISE: A Phase 3 randomized trial of erenumab for episodic
migraine. _Cephalalgia_ 38, 1026–1037. https://doi.org/10.1177/0333102418759786 (2018). Article PubMed Google Scholar * Martelletti, P. _et al._ My migraine voice survey: A global study
of disease burden among individuals with migraine for whom preventive treatments have failed. _J. Headache Pain_ 19, 115. https://doi.org/10.1186/s10194-018-0946-z (2018). Article PubMed
PubMed Central Google Scholar * Radtke, A. & Neuhauser, H. Low rate of self-awareness and medical recognition of migraine in Germany. _Cephalalgia_ 32, 1023–1030.
https://doi.org/10.1177/0333102412454945 (2012). Article CAS PubMed Google Scholar * Lucas, C., Geraud, G., Valade, D., Chautard, M. H. & Lanteri-Minet, M. Recognition and
therapeutic management of migraine in 2004, in France: Results of FRAMIG 3, a French nationwide population-based survey. _Headache_ 46, 715–725.
https://doi.org/10.1111/j.1526-4610.2006.00430.x (2006). Article PubMed Google Scholar * Young, W. B., Park, J. E., Tian, I. X. & Kempner, J. The stigma of migraine. _PLoS ONE_ 8,
e54074. https://doi.org/10.1371/journal.pone.0054074 (2013). Article ADS CAS PubMed PubMed Central Google Scholar * Kavuk, I. _et al._ One-year prevalence and socio-cultural aspects of
chronic headache in Turkish immigrants and German natives. _Cephalalgia_ 26, 1177–1181. https://doi.org/10.1111/j.1468-2982.2006.01186.x (2006). Article CAS PubMed Google Scholar *
Steiner, T. J. _et al._ Headache service quality: The role of specialized headache centres within structured headache services, and suggested standards and criteria as centres of excellence.
_J. Headache Pain_ 20, 24. https://doi.org/10.1186/s10194-019-0970-7 (2019). Article CAS PubMed PubMed Central Google Scholar * Starling, A. J. & Dodick, D. W. Best practices for
patients with chronic migraine: Burden, diagnosis, and management in primary care. _Mayo Clin. Proc._ 90, 408–414. https://doi.org/10.1016/j.mayocp.2015.01.010 (2015). Article PubMed
Google Scholar * Diener, H. C., Solbach, K., Holle, D. & Gaul, C. Integrated care for chronic migraine patients: Epidemiology, burden, diagnosis and treatment options. _Clin. Med.
(Lond.)_ 15, 344–350. https://doi.org/10.7861/clinmedicine.15-4-344 (2015). Article Google Scholar * Diener, H.-C., Gaul, C., Kropp, P. et al., Therapie der Migräneattacke und Prophylaxe
der Migräne, S1-Leitlinie. _Deutsche Gesellschaft für Neurologie (Hrsg.)_ Leitlinien für Diagnostik und Therapie in der Neurologie (2018). * Hepp, Z. _et al._ Persistence and switching
patterns of oral migraine prophylactic medications among patients with chronic migraine: A retrospective claims analysis. _Cephalalgia_ 37, 470–485. https://doi.org/10.1177/0333102416678382
(2017). Article PubMed Google Scholar * Lipton, R. B. _et al._ A self-administered screener for migraine in primary care: The ID Migraine validation study. _Neurology_ 61, 375–382.
https://doi.org/10.1212/01.wnl.0000078940.53438.83 (2003). Article CAS PubMed Google Scholar * Thiele, A., Strauß, S., Angermaier, A., Kronenbuerger, M. & Fleischmann, R. Translation
and validation of an extended German version of ID Migraine™ as a migraine screening tool. _Cephalalgia Rep._ 3, 2515816320962773. https://doi.org/10.1177/2515816320962773 (2020). Article
Google Scholar Download references ACKNOWLEDGEMENTS The authors wish to thank all participants in this study for their contribution, Dr. Daniela Mailänder-Sánchez and Dr. Antje Tunger
(medizinwelten-services GmbH, Stuttgart, Germany) for technical editing of the manuscript, and Dr. Diane Milburn (Alnwick, UK) for language and editorial support. The Figures were produced
by Marie Groth, one of the authors of this manuscript. FUNDING This study was sponsored by Novartis Pharma GmbH, Nuremberg, Germany. Novartis sponsored the data collection, data analysis,
manuscript development, submission as well as technical editing and language editing assistance. AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Novartis Pharma GmbH, Nuremberg, Germany Marie
Groth & Marc Ehrlich * Evangelical Hospital Unna, Unna, Germany Zaza Katsarava * Department of Neurology, University of Duisburg-Essen, Essen, Germany Zaza Katsarava * EVEX Medical
Corporation, Tbilisi, Republic of Georgia Zaza Katsarava * IM Sechenov First Moscow State Medical University (Sechenov University), Moscow, Russian Federation Zaza Katsarava Authors * Marie
Groth View author publications You can also search for this author inPubMed Google Scholar * Zaza Katsarava View author publications You can also search for this author inPubMed Google
Scholar * Marc Ehrlich View author publications You can also search for this author inPubMed Google Scholar CONTRIBUTIONS Z.K. and M.E. designed the study; Z.K., M.E. and M.G. analysed and
interpreted the results and developed and prepared the manuscript. All authors read and approved the final manuscript and are accountable for their contribution to the work. CORRESPONDING
AUTHOR Correspondence to Marc Ehrlich. ETHICS DECLARATIONS COMPETING INTERESTS ZK received research funding from Novartis. He received consultation fees from Allergan, Daiichi, Lilly,
Lundbeck, Merck, Novartis, TEVA. None of them were related to this work. MG and ME are Novartis employees. ADDITIONAL INFORMATION PUBLISHER'S NOTE Springer Nature remains neutral with
regard to jurisdictional claims in published maps and institutional affiliations. SUPPLEMENTARY INFORMATION SUPPLEMENTARY INFORMATION. RIGHTS AND PERMISSIONS OPEN ACCESS This article is
licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give
appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in
this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's
Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder.
To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Groth, M., Katsarava, Z. & Ehrlich, M.
Results of the gErman migraine PatIent Survey on medical Care and prOPhylactic treatment Experience (EPISCOPE). _Sci Rep_ 12, 4589 (2022). https://doi.org/10.1038/s41598-022-08716-w Download
citation * Received: 28 June 2021 * Accepted: 07 March 2022 * Published: 17 March 2022 * DOI: https://doi.org/10.1038/s41598-022-08716-w SHARE THIS ARTICLE Anyone you share the following
link with will be able to read this content: Get shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature
SharedIt content-sharing initiative
Trending News
Kitchen sink: basin of information👮♂️ THE SPRINGDALE POLICE chief plans to retire next year. (_Northwest Arkansas Democrat-Gazette)_ 🎥 A NEW MOVIE — a We...
Rural crime wave hits scotland, wales and northern ireland - farmers weeklyFARMERS IN Northern Ireland, Wales and Scotland need to tighten up their security because the regions are fast becoming ...
Kids now spend nearly as much time watching tiktok as youtube in us, uk and spain | techcrunchA new study on kids’ app usage and habits indicates a major threat to YouTube’s dominance, as kids now split their time ...
Co-operation in Bibliography | NatureABSTRACT THE movement for co-operation in bibliography has received an important impetus from the Bataafsche Petroleum M...
Robert f. Kennedy jr. Wants to get on the ballot in all 50 states. It won't be easyWith many Americans unhappy at the prospect of a rematch between President Biden and former President Donald Trump, vote...
Latests News
Results of the german migraine patient survey on medical care and prophylactic treatment experience (episcope)ABSTRACT Migraine affects about 12% of the worldwide population causing substantial personal and societal burden. Yet, m...
Soul stereo - rub a dub party #20 @cabaret sauvageDirection le Cabaret Sauvage, le 6 février 2015, pour une Soul Stereo. A l'occasion de l'anniversaire des 70 a...
The page you were looking for doesn't exist.You may have mistyped the address or the page may have moved.By proceeding, you agree to our Terms & Conditions and our ...
Opportunities to maximise the benefits of motorcycle and motorised three-wheeler taxis in rural democratic republic of congo, policy briefOPPORTUNITIES TO MAXIMISE THE BENEFITS OF MOTORCYCLE AND MOTORISED THREE-WHEELER TAXIS IN RURAL DEMOCRATIC REPUBLIC OF C...
The hidden curriculum of higher educationMay 1 is the national deposit deadline for colleges and universities. This is the day when students make their final col...