Global Variation of Nutritional Status in Children Undergoing Chronic Peritoneal Dialysis: A Longitudinal Study of the International Pediatric Peritoneal Dialysis Network
Global Variation of Nutritional Status in Children Undergoing Chronic Peritoneal Dialysis: A Longitudinal Study of the International Pediatric Peritoneal Dialysis Network"
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
While children approaching end-stage kidney disease (ESKD) are considered at risk of uremic anorexia and underweight they are also exposed to the global obesity epidemic. We sought to
investigate the variation of nutritional status in children undergoing chronic peritoneal dialysis (CPD) around the globe. The distribution and course of body mass index (BMI) standard
deviation score over time was examined prospectively in 1001 children and adolescents from 35 countries starting CPD who were followed in the International Pediatric PD Network (IPPN)
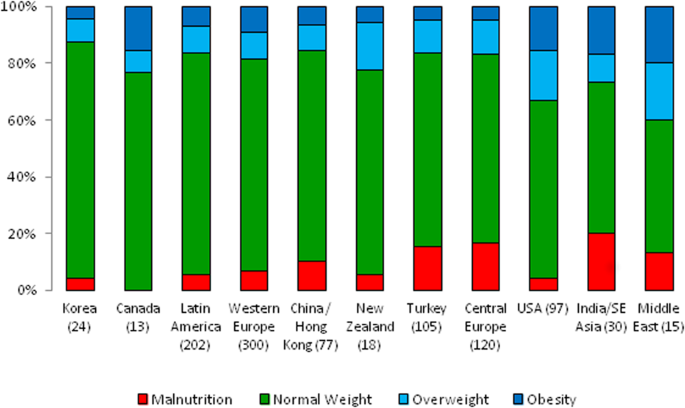
Registry. The overall prevalence of underweight, and overweight/obesity at start of CPD was 8.9% and 19.7%, respectively. Underweight was most prevalent in South and Southeast Asia (20%),
Central Europe (16.7%) and Turkey (15.2%), whereas overweight and obesity were most common in the Middle East (40%) and the US (33%). BMI SDS at PD initiation was associated positively with
current eGFR and gastrostomy feeding prior to PD start. Over the course of PD BMI SDS tended to increase on CPD in underweight and normal weight children, whereas it decreased in initially
overweight patients. In infancy, mortality risk was amplified by obesity, whereas in older children mortality was markedly increased in association with underweight. Both underweight and
overweight are prevalent in pediatric ESKD, with the prevalence varying across the globe. Late dialysis start is associated with underweight, while enteral feeding can lead to obesity.
Nutritional abnormalities tend to attenuate with time on dialysis. Mortality risk appears increased with obesity in infants and with underweight in older children.
The nutritional status is a principal concern when caring for children undergoing chronic peritoneal dialysis (CPD). While early studies revealed providing sufficient nutrition was essential
for adequate growth in this population, advances in enteral feeding practices have enabled the elimination of underweight but have not improved linear growth as much as expected1,2,3.
Recent concerns have emerged on the potential for adverse effects of excessive caloric intake in patients who receive supplemental feeding1,2,3.
The majority of published studies assessing the nutritional status of dialyzed children were performed at highly specialized pediatric dialysis units in North America and Western Europe. In
contrast, on a global scale the risk of nutritional abnormalities in individual regions and countries is likely to be affected by a range of medical and non-medical factors including the
patient case-mix regarding age, underlying disease and co-morbidities, national economic strength and healthcare expenditure, cultural acceptability of dietary and feeding prescriptions,
availability of special formula diets and enteral feeding equipment, and differences in local, national or regional nutritional recommendations4.
The International Pediatric Peritoneal Dialysis Network (IPPN) has been collecting comprehensive clinical and laboratory data in a standardized manner from children undergoing CPD worldwide
since 2007. Since these data include detailed anthropometric measures, feeding prescriptions and outcome measures, it provides an opportunity to address the global demographics of
nutritional abnormalities in children receiving CPD.
The objective of this study was to examine and follow prospectively the nutritional status of 1,001 children commencing CPD around the globe, analyze factors associated with the nutritional
status at the start and during the course of dialysis, and to analyze the impact of nutritional abnormalities on patient survival.
The IPPN Registry was established in 2007 and currently collects comprehensive clinical and laboratory information from children undergoing CPD at 95 pediatric dialysis centers in 37
countries around the globe. Patient status is updated every 6 months via an Internet-based web platform (www.pedpd.org). The complete list of data items collected has been published
previously2,4. Data is automatically checked for plausibility and completeness. Data protection is ensured by pseudonymized data input. The study is performed in accordance with the relevant
medical association’s professional codes of conduct with the Declaration of Helsinki from 2008. Approval for the registry project was obtained from The Children’s Mercy Hospital Pediatric
Institutional Review Board, Kansas City, USA and local Institutional Review Boards or ethical committees. Informed consent was obtained from the patients and/or their legal guardians as
required by local review boards.
Body Mass Index (BMI), i.e. weight/height2 (kg/m2), was normalized to standard deviation scores (SDS) according to height age, utilizing the WHO (2006) and CDC (2000) standards for children
aged younger and older than 5 years, respectively (see www.who.int/childgrowth/en/)5,6. Normalization to height age, i.e. the chronological age of a child with the same height growing at the
50th height percentile, was made to adjust for the high prevalence of growth failure in the cohort7. BMI SDS values were used to categorize patients into three BMI groups: underweight
(1.036 to 1.645 SDS), and obesity (>95th percentile, i.e. >1.645 SDS). The Schwartz bedside formula was used to estimate GFR at initiation of CPD8.
Data collection was complete for all observations except residual urine output (7.6% missing data), daily ultrafiltration rate (5.2%), eGFR (1.2%), total PD fluid turnover and dialytic
glucose exposure (0.8%), PD modality (0.5%), serum bicarbonate (0.3%), serum albumin (0.2%), and estimated dry weight (0.2%). Multiple imputation by chained equations was conducted to
replace these missing values9. All analyses were performed using the imputed dataset. Additionally, sensitivity analyses were performed using only cases with complete data sets.
ANOVA or Kruskal-Wallis tests were conducted to compare differences between BMI groups. Differences in proportions were assessed using Chi2 tests. Linear mixed modeling was used to identify
factors affecting BMI SDS at baseline and during follow-up. The initial cross sectional model included age, sex, eGFR, gross national income (GNI), renal diagnosis, presence of
comorbidities, ethnicity, urine output, nutritional support (oral caloric supplements, nasogastric tube (NGT) and gastrostomy feeding), and growth hormone use as independent variables. The
region of residence was accounted for as random intercept. For the longitudinal analysis, the change in BMI SDS between two observations, projected to 12 months, was used as the dependent
variable and region and patients were used as nested random effects. Potential covariates included in the initial model were age at baseline, sex, presence of comorbidities, renal diagnosis,
GNI and the time-varying variables BMI SDS, height SDS, eGFR, % deviation from estimated dry weight, PD modality, duration of PD, serum albumin, serum bicarbonate, total PD fluid volume,
urine output, ultrafiltration, growth hormone use, nutritional support, glucose exposure, biocompatible PD fluid use, and amino acid PD fluid use. A stepwise variable selection procedure was
applied to identify the relevant covariates for the cross sectional model as well as for the longitudinal model, using p = 0.2 as a cutoff criterion for model entry.
Kaplan–Meier analysis with log-rank testing was used to assess differences in patient survival. Cox proportional hazard modeling with time dependent covariates and interaction term was
applied to identify risk factors of death on dialysis.
Data were analyzed using SAS, version 9.3 (SAS Institute, Inc., Cary, NC), and R, version 3.1.110.
All children and adolescents enrolled in the IPPN registry with initiation of CPD between March 2007 and December 2014 were analyzed for this study. Five patients with syndromic and
metabolic disorders associated with intrinsic abnormalities of growth and body composition were excluded from the analysis. The final dataset comprised a total of 1,001 incident patients
from 85 nephrology centers in 35 countries. Children originated from Western Europe (n = 300), Central Europe (n = 120), Turkey (n = 105), the Middle East (n = 15), China and Hong Kong (n =
77), Korea (n = 24), India and South East Asia (n = 30), New Zealand (n = 18), USA (n = 97), Canada (n = 13) and Latin America (n = 202). One or more comorbidities were reported in 369
patients (35.6%); these included mainly defined syndromic disorders (n = 107), impaired cognitive development (n = 119), cardiac (n = 130) and pulmonary abnormalities (n = 52).
Of the 1,001 patients, 702 (70%) patients had at least two BMI records available. Median follow-up time was 14.5 (IQR 17.8) months. Altogether, the data set contained 2,931 follow-up
entries.
The overall prevalence of underweight, normal weight and overweight/obesity at the start of CPD was 8.9%, 71.4%, and 19.7%, respectively. The detailed patient characteristics according to
nutritional status at dialysis entry are shown in Table 1. Overweight/obese children originated from countries with higher GNI per capita, had higher eGFR at CPD initiation and were more
growth retarded. Gastrostomy feeding was performed in almost 17% of the overweight children as compared to 8% and 6% in the normal and low BMI groups (p
Trending News
Un human rights council 45: interactive dialogue with the fact finding mission on venezuelaSpeech UN HUMAN RIGHTS COUNCIL 45: INTERACTIVE DIALOGUE WITH THE FACT FINDING MISSION ON VENEZUELA UK's Internation...
Roger cohen: why obama should visit a mosque------------------------- * * X.com * Facebook * E-Mail * * * X.com * Facebook * E-Mail * Messenger * WhatsApp * Dieser ...
Gateway Communications OKs Reverse Stock SplitGateway Communications Inc. said it will ask shareholders to approve a one-for-200 reverse stock split at the company’s ...
Goa: Apex Court sets aside Green Tribunal order to demolish Curlie’sThe Supreme Court of India set aside the order of the National Green Tribunal (NGT) that had ordered the demolition of C...
Page not found - Eenadu.netTRENDING IPL 2025 Rains Breaking | Feedback | ePratibha | E-PAPER | Pratibha ఆంధ్రప్రదేశ్ రాష్ట్ర వార్తలు జిల్లా వార్తలు...
Latests News
Global Variation of Nutritional Status in Children Undergoing Chronic Peritoneal Dialysis: A Longitudinal Study of the International Pediatric PeritonWhile children approaching end-stage kidney disease (ESKD) are considered at risk of uremic anorexia and underweight the...
Valuation office agency: november 2016 transparency dataTransparency data VALUATION OFFICE AGENCY: NOVEMBER 2016 TRANSPARENCY DATA The Valuation Office Agency (VOA) publishes a...
Regulatory article (ra) 3205: radar analysis cellRegulation REGULATORY ARTICLE (RA) 3205: RADAR ANALYSIS CELL RA covering services to support the joint and integrated ap...
'i'm a sunbed warrior - i'll reserve with a towel and go to breakfast'RACHEL MCGUIGAN AND HER HUSBAND DAVID DECIDED TO RESERVE THEIR SUNBEDS WITH TOWELS BEFORE GOING OFF TO BREAKFAST - BUT I...
DNA Edit: Battle for PresidencyBy the 25th of July, India will have its 14th President, after a contest, which by the looks of it can either go down to...