Clinical features of intratarsal keratinous cysts
Clinical features of intratarsal keratinous cysts"
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT PURPOSE Intratarsal keratinous cysts (IKCs) have been frequently misdiagnosed as chalazia or epidermal cysts. We reviewed a series of cases of IKCs to identify clinical features
that distinguish IKCs from other eyelid diseases. METHODS We retrospectively reviewed the medical records of 17 suspected IKC patients between January 2004 and September 2014. RESULTS
Seventeen patients who were clinically suspected to have IKC were enrolled. All patients presented with non-inflamed eyelid nodules fixed to the tarsus. Among them, 12 biopsy specimens were
available and 11 patients (91.7%) were diagnosed with IKC, with a pathological finding of stratified squamous cell lining with keratin material. The mean patient age was 55.1 years (31–71).
Six patients had a surgical history of incision or incomplete excision of the lesion, followed by recurrence. On eyelid eversion, five patients showed a white–yellow nodule, and three
patients had a bluish cystic lesion. The diameter of the nodules ranged from 4 to 10 mm. The intracystic material was a milky white fluid. Ten patients underwent a complete surgical excision
including partial tarsectomy and there was no recurrence. CONCLUSIONS IKC can be distinguished from other intratarsal lesions by a characteristic tarsal nodule fixed to the tarsus. To
prevent recurrence, complete excision with partial tarsectomy is needed. SIMILAR CONTENT BEING VIEWED BY OTHERS THE SURGICAL MANAGEMENT AND OUTCOMES OF KISSING NEVI OF THE EYELIDS Article 11
March 2023 A RETROSPECTIVE STUDY OF CONJUNCTIVAL LESIONS IN THE PAEDIATRIC EYE CLINIC OVER 12 YEARS Article 26 September 2023 COMPARISON OF THREE SURGICAL TECHNIQUES FOR INTERNAL ANGULAR
DERMOID CYSTS: A RANDOMIZED CONTROLLED TRIAL Article 20 November 2021 INTRODUCTION Most common primary intratarsal lesions are chalazia and sebaceous gland carcinomas.1 An intratarsal
keratinous cyst (IKC), recently described by Jakobiec _et al_,2 is an intratarsal mass lesion that originates from the meibomian glands or their ducts. Importantly, IKC has been frequently
misdiagnosed as chalazion or other benign eyelid cystic tumors because it is an intratarsal hard nodular mass. It is important to differentiate IKC from other eyelid intratarsal lesions
because its therapeutic approach and clinical outcomes are quite different; IKC has to be completely excised with partial tarsectomy. In contrast, a chalazion is easily treated with a simple
incision and curettage (I&C). Sebaceous gland carcinomas often metastasize and contribute to mortality despite radical surgical excision. Some reports3, 4 have highlighted the
histopathological features of IKC. However, there is no published report of the correlation between clinically suspected IKC and confirmed diagnosis of IKC by pathological examination. In
this study, we report on 11 cases of histologically confirmed IKC and their clinical features. MATERIALS AND METHODS Patients who underwent surgical treatment for eyelid masses at four
different medical centers from January 2004 to September 2014 were recruited, and their medical records and photographs were retrospectively reviewed. The records of patients who were
assumed to have IKC were collected and their pathologic slides were re-examined by an experienced pathologist (CL). The data included sex, age at the time of excision, location, color and
size of the lesions, related symptoms, duration of symptoms, findings on external examination and eyelid eversion, previous diagnosis, treatment, intraoperative findings, previous history of
treatment, follow-up duration, and recurrence. This study complied with the Declaration of Helsinki guidelines and was approved by the Institutional Review Board of Seoul Metropolitan
Government Seoul National University Boramae Medical Center, Seoul, Korea. RESULTS Seventeen patients who were clinically suspected to have IKC were enrolled. All patients presented with
non-inflamed firm nodules fixed to the tarsus. Among them, the biopsy specimens of 12 patients were available and 11 patients (91.7%) were given a confirmed diagnosis of IKC by pathological
examination (Table 1). The mean patient age was 55.1 years (range 31–71 years), and five patients were men and six were women. The overlying skin was freely movable without focal adhesion.
All mass lesions were located at the upper eyelid. On eyelid eversion, well-demarcated upraised intratarsal lesions were found through the conjunctiva, and the surrounding conjunctiva was
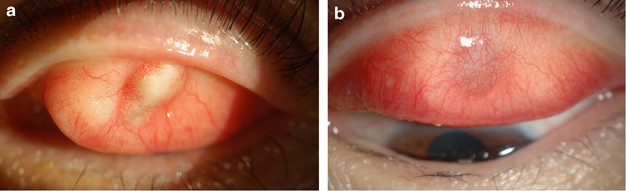
not inflamed. The nodules had a diameter of ~4–10 mm, with a mean diameter of 6.6 mm (Table 1). Five patients showed a white to yellow nodular bulge and three patients showed a bluish cystic
lesion (Figure 1). All IKCs were solitary except one in which multiple lesions distorted the eyelid margin. One clinically misdiagnosed patient was diagnosed as having an epidermal cyst.
Six patients had a history of incision or incomplete excision followed by recurrence. Previously, before recognition of IKC as an entity, patients were clinically diagnosed as having another
disease; two patients as having a chalazion, three patients as having an epidermal cyst, and four patients as having a tarsal mass. Pathological examination, which was performed on 12
patients prior to the discovery of IKC, indicated that 3 patients had an epidermal inclusion cyst, 3 patients had a steatocystoma, 2 patients had a keratinous cyst, 1 patient had a cyst of
Moll’s gland, 1 patient had a pilar cyst, and 1 patient had a benign cyst with fibrovascular tissue. After review by an experienced pathologist, all cases except one were re-diagnosed as IKC
(Figure 2). Ten patients underwent surgical excision including partial tarsectomy: four patients through a transcutaneous approach, four patients through a transconjunctival approach, and
two patients through an unrecorded approach. We did not suture the conjunctiva after using the transconjunctival approach and there were no corneal complications. Six cases were ruptured
during dissection and a milk-like fluid mixed with solid elements having the consistency of tofu residue, which is different from the ordinary content of chalazia, was extruded. None of the
patients experienced recurrence during the follow-up, which had a mean duration of 5 weeks (range, 1–24 weeks). Among the 12 patients who were clinically suspected as having IKC, only one
patient was ultimately pathologically diagnosed with an epidermal cyst. In this patient, an intratarsal gray–black mass was also observed on eyelid eversion. However, on pathological
examination, the cyst was lined by focal acanthotic squamous epithelium and had a granular layer in the cyst wall. Thus, these findings were indicative of an epidermal cyst, rather than IKC.
DISCUSSION IKCs are a recently described entity that arises from the Meibomian glands and are thought to be the third major cause of intratarsal swelling after chalazia and sebaceous cell
carcinomas.2 The clinical characteristics of IKCs are similar to those of chalazia and epidermal inclusion cysts, but there are differentiating features that enable physicians to distinguish
them. For example, lesions such as steatocystomas and pilomatrixomas are white to yellow, as are IKCs. In contrast, although chalazia are fixed to the tarsus similarly to IKC, they are
frequently accompanied by surrounding inflammation and the margin of the lesion is less clear than that of an IKC. These features are helpful for differentiation of chalazia from IKC.5 An
epidermal inclusion cyst is a non-inflammatory, palpable nodule that is not fixed to the tarsus but is freely movable, which is another differentiating characteristic with regard to IKC.6
The cyst content of a steatocystoma is a yellowish oily sebum containing hair shafts, and steatocystomas are not attached to the tarsus.7 Only two cases of pilomatrixoma observed at the
tarsal conjunctiva have been reported.8, 9 Usually, pilomatrixoma grows toward the skin and is freely movable from the tarsus because it is thought to originate from hair follicle cells.
Furthermore, patients with pilomatrixoma are usually young, and hyperemia is observed surrounding the lesion, in contrast to IKC. IKCs occasionally have a blue–gray color because of the
Tyndall effect, and a blue IKC is occasionally misdiagnosed as melanoma.2 As awareness of IKC increases, histopathological differences between this entity and other diseases are being
revealed. Even though IKC and steatocystoma share similar histological findings, such as trichilemmal keratinization, steatocystomas contain sebaceous glands in the cyst wall or adjoining
wall. However, for most cases, a careful clinical examination can provide sufficient evidence for a differential diagnosis. With the aforementioned clinical characteristics in mind, we
reviewed medical photographs and records to identify cases that were previously diagnosed as chalazia or epidermal cysts and were now clearly re-diagnosed as IKC. As a result, among 12
patients who were clinically suspected as having IKC, only one patient was ultimately pathologically diagnosed with an epidermal cyst. Previously, IKC was a commonly misdiagnosed lesion.
However, with further investigation, we found that most cases were correctly diagnosed as IKC. Regarding pathogenesis, Lucarelli _et al_10 suggested that eyelid surgery or trauma may cause a
blockage of the tarsal sebaceous ducts and squamous metaplasia, leading to the development of IKCs. In our study, there were eight cases of tarsal nodule excision or incision and one case
of a double eyelid operation, which occurred ~23 years ago. However, Jakobiec _et al_2 reported that IKC consists of a firm fibrous cyst and intracystic content, and that the fibrous wall of
the cyst is composed of tightly woven bundles of collagen. They also reported that the ducts and ductules of the Meibomian glands were composed of non-keratinizing squamous epithelium, and
there was no histological evidence of squamous metaplasia. Therefore, we did not exclude the patient who had a previous double eyelid operation from this study. In our study, there was one
case with multiple lesions. In 2012, Kim _et al_11 reported multiple IKCs of the eyelid for the first time. Subsequently, to our knowledge, there has been no report of multiple IKCs, and
thus, we assume that multiple IKCs are uncommon. Furthermore, we could not find a cause for the multiple cysts in our case, which is consistent with the case of Kim _et al_ Further
observation would be needed to understand the mechanism of multiple lesions. Therapeutically, it is important to distinguish IKC from other similar lesions because IKC requires complete
excision. There are many cases of multiple recurrences that were previously diagnosed as chalazia and subsequently operated on with an incomplete excision or I&C. The multiple
recurrences of chalazia suggest that the diagnosis was incorrect. To excise an IKC, a partial tarsectomy is mandatory because of its firm adhesion to the tarsus, and this procedure that will
remarkably reduce recurrence.2 Surgically, there are following two approaches: transcutaneous and transconjunctival. Patel _et al_3 reported that an anterior lid crease approach with full
excision of the intratarsal cyst and partial excision of the underlying anterior tarsus is effective for preventing local recurrence and avoiding more complex lid reconstruction. In
addition, Zhang _et al_4 suggested that a transconjunctival incision avoids an eyelid incision and disfiguration. They suggested that because the IKC is fixed to the tarsus and is
independent of the skin, the conjunctival approach with partial tarsectomy is a better way to excise the entire lesion and simultaneously avoid cosmetic problems. Comparisons of
transconjunctival _vs_ transcutaneous approaches for lower eyelid blepharoplasty or orbit wall fracture repair have been studied previously. However, no report has identified a better
approach for tarsal lesions. In our study, there were four cases with a transcutaneous approach and four cases with a transconjunctival approach, and no patients reported dissatisfaction
with the cosmetic outcomes. There was also no case of severe eyelid contour distortion or scar formation. In this study, we identified 11 cases of IKC and their clinical features. It is
important to distinguish IKC from other similar lesions because IKC requires complete excision. The results indicate that multiple recurrences after I&C or incision and drainage of a
non-inflammatory, painless intratarsal mass suggest the presence of IKC. REFERENCES * Spencer WH . _Ophthalmic Pathology: an Atlas and Textbook_, 4th edn. WB Saunders: Philadelphia, PA, USA,
1996; 2378–2380. Google Scholar * Jakobiec FA, Mehta M, Iwamoto M, Hatton MP, Thakker M, Fay A . Intratarsal keratinous cysts of the Meibomian gland: distinctive clinicopathologic and
immunohistochemical features in 6 cases. _Am J Ophthalmol_ 2010; 149 (1): 82–94. Article Google Scholar * Patel VS, Meyer DR, Carlson JA . Intratarsal keratinous cysts of the meibomian
gland (a sebaceous duct cyst): report of 2 cases. _Am J Dermatopathol_ 2011; 33 (6): 624–627. Article Google Scholar * Zhang ZD, Li X, Li M, Zhao J, Zhou KJ, Qu J . Clinicopathological
features and surgical treatment of intratarsal keratinous cysts. _Am J Dermatopathol_ 2013; 35 (1): 78–82. Article Google Scholar * Dhaliwal U, Arora VK, Singh N, Bhatia A . Cytopathology
of chalazia. _Diagn Cytopathol_ 2004; 31 (2): 118–122. Article Google Scholar * Dutton JJ, Fowler AM, Proia AD . Dermoid cyst of conjunctival origin. _Ophthal Plast Reconstr Surg_ 2006; 22
(2): 137–139. Article Google Scholar * Procianoy F, Golbert MB, Golbspan L, Duro KM, Bocaccio FJ . Steatocystoma simplex of the eyelid. _Ophthal Plast Reconstr Surg_ 2009; 25 (2):
147–148. Article Google Scholar * de Azevedo ML, Milani JA, de Souza EC, Nemer RS . Pilomatrixoma. An unusual case with secondary corneal ulcer. _Arch Ophthalmol_ 1985; 103 (4): 553–554.
Article CAS Google Scholar * Monshizadeh R, Cohen L, Rubin PA . Perforating follicular hybrid cyst of the tarsus. _J Am Acad Dermatol_ 2003; 48 (2 Suppl): S33–S34. Article Google Scholar
* Lucarelli MJ, Ahn HB, Kulkarni AD, Kahana A . Intratarsal epidermal inclusion cyst. _Ophthal Plast Reconstr Surg_ 2008; 24 (5): 357–359. Article Google Scholar * Kim HJ, Wojno TH,
Grossniklaus HE . Multiple intratarsal keratinous cysts of the eyelid. _Ophthal Plast Reconstr Surg_ 2012; 28 (5): e116. Article Google Scholar Download references AUTHOR INFORMATION
AUTHORS AND AFFILIATIONS * Department of Ophthalmology, Seoul National University College of Medicine, Seoul, Korea J A Kim & S I Khwarg * Department of Ophthalmology, Seoul National
University Bundang Hospital, Seongnam, Korea N Kim * Department of Ophthalmology, Seoul Metropolitan Government–Seoul National University Boramae Medical Center, Seoul, Korea H-K Choung *
Department of Ophthalmology, Hallym University Sacred Heart Hospital, Anyang, Korea M J Lee * Department of Pathology, Seoul National University College of Medicine, Seoul, Korea C Lee
Authors * J A Kim View author publications You can also search for this author inPubMed Google Scholar * N Kim View author publications You can also search for this author inPubMed Google
Scholar * H-K Choung View author publications You can also search for this author inPubMed Google Scholar * M J Lee View author publications You can also search for this author inPubMed
Google Scholar * C Lee View author publications You can also search for this author inPubMed Google Scholar * S I Khwarg View author publications You can also search for this author inPubMed
Google Scholar CORRESPONDING AUTHOR Correspondence to H-K Choung. ETHICS DECLARATIONS COMPETING INTERESTS The authors declare no conflict of interest. ADDITIONAL INFORMATION This paper has
not been presented in any academic conference. RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Kim, J., Kim, N., Choung, HK. _et al._ Clinical features
of intratarsal keratinous cysts. _Eye_ 30, 59–63 (2016). https://doi.org/10.1038/eye.2015.184 Download citation * Received: 02 March 2015 * Accepted: 25 July 2015 * Published: 02 October
2015 * Issue Date: January 2016 * DOI: https://doi.org/10.1038/eye.2015.184 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get shareable link
Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative
Trending News
Aarp vital voices: consumer fraud among u. S. Adults ages 45+: incidence, concern, protection, vulnerabilityThe Federal Trade Commission’s (FTC) 2020 Consumer Sentinel Report shows U.S. consumers filed more than 4.7 million repo...
How will the ukraine crisis play out in british politics? | thearticleToday had been billed as the day of reckoning in Ukraine. At the time of writing, reports of a Russian withdrawal have d...
Observation of an acoustic octupole topological insulatorABSTRACT Berry phase associated with energy bands in crystals can lead to quantised observables like quantised dipole po...
Cristiano ronaldo – latest news information updated on may 29, 2025 | articles & updates on cristiano ronaldo | photos & videos | latestlyCristiano Ronaldo – Latest News Information updated on May 29, 2025 | Articles & Updates on Cristiano Ronaldo | Phot...
Four things you should never put in a textMemorial Day Sale! Join AARP for just $11 per year with a 5-year membership Join now and get a FREE gift. Expires 6/4 G...
Latests News
Clinical features of intratarsal keratinous cystsABSTRACT PURPOSE Intratarsal keratinous cysts (IKCs) have been frequently misdiagnosed as chalazia or epidermal cysts. W...
Univeristy and educational intelligenceABSTRACT CAMBRIDGE.—J. A. Ratecliffe, Stokes student of Pembroke College formerly research student of Sidney Sussex Coll...
Every person in scotland has played their part in this national endeavour — scottish national partyTACKLING COVID-19 HAS TRULY BEEN A NATIONAL ENDEAVOUR, WITH EVERY PERSON IN SCOTLAND PLAYING THEIR PART. Scotland’s key ...
William Hague | TheArticleFirst {{register.errors.names}} Last Gender What's this for? Age bracket What's this for? This is to help us s...
Nursing home covid deaths increasing this winterThe federal government contracted with CVS, Walgreens and some other pharmacies to conduct on-site vaccine clinics at ...