Upper thoracic disc herniation followed by acutely progressing paraplegia
Upper thoracic disc herniation followed by acutely progressing paraplegia"
- Select a language for the TTS:
- UK English Female
- UK English Male
- US English Female
- US English Male
- Australian Female
- Australian Male
- Language selected: (auto detect) - EN
Play all audios:
ABSTRACT STUDY DESIGN: Case report. OBJECTIVE: To report a rare thoracic intervertebral disc herniation followed by acutely progressing paraplegia. SETTING: Spinal Injuries Center, Fukuoka,
Japan. METHOD: A 37-year-old man presented with sudden severe backache and acutely progressing motor impairments of both lower extremities after antecedent backache lasting about 5 days.
Neurological examination showed analgesia and hypoesthesia below the T4 dermatome level, dysesthesia to pinprick below right inguinal level, and severe motor impairments of the lower
extremities (Frankel classification C). Magnetic resonance (MR) imaging demonstrated spinal cord compression due to a postero-laterally existing epidural mass at the T2–T3 level. After
laminectomy at the T2–T3 level, the sequestrated disc material was detected and excised as one piece through the right side of the dura. The excised herniated mass had a ring-like form and
was thought to originate from the annulus fibrosis. RESULT: After the emergency surgery, he had complete relief from the backache and control of both lower extremities recovered gradually.
At 4 weeks after the emergent operation, motor power of both lower extremities recovered almost completely. He was able to walk without any assistance. MR imaging study after surgery did not
reveal the sequestrated mass, except for a mild disc bulging at the T2–T3 level. CONCLUSION: Accurate diagnosis of acute symptomatic thoracic disc herniation is occasionally difficult.
However, timely and successful surgery could result in complete symptom relief and satisfactory results. SIMILAR CONTENT BEING VIEWED BY OTHERS POSTERIOR EPIDURAL SEQUESTRATED DISC
PRESENTING WITH CONTRALATERAL RADICULOPATHY: A VERY RARE CASE Article 06 November 2021 SPINAL CORD DISORDER DUE TO SPINAL EPIDURAL ABSCESS SECONDARY TO THORACIC FACET JOINT SEPTIC
ARTHRITIS—A RARE CASE WITH A SURPRISING EVOLUTION Article 19 November 2020 NATURAL HISTORY AND SURGICAL OUTCOMES OF IDIOPATHIC SPINAL CORD HERNIATION Article 28 June 2023 INTRODUCTION
Thoracic disc herniations are rare compared with herniations at cervical or lumbar disc levels, and they are mainly located at a lower thoracic level.1 When it does occur, symptomatic
thoracic disc herniation is a slowly progressive disease.2 To our knowledge, acutely developing disc herniation at the upper thoracic level has not been previously reported in the English
literature. We describe a case of the upper thoracic disc herniation (T2–T3) with rapidly progressing paraplegia due to a dorsally sequestrated herniated disc, which could be successfully
removed by posterior surgery. CASE REPORT PRESENTATION A previously healthy 37-year-old man (height: 177 cm, weight: 100 kg) presented with a sudden backache and motor impairments of both
lower extremities after antecedent backache lasting for about 5 days. He did not report any previous trauma. Motor impairments of both lower extremities deteriorated gradually, and about 3 h
after the onset of the motor impairments, he could not stand without assistance. He was admitted to another hospital and magnetic resonance (MR) imaging study of the whole spine was
performed, revealing compression of the thoracic spinal cord at the T2–T3 level. At 6 h after the onset of motor impairments, he was transferred to our hospital. EXAMINATION On physical
examination, there was tenderness in the upper part of the back. He did not have fever. On neurological examination, hyperreflexia of both lower extremities was observed and both Babinski
reflexes were positive. He had analgesia and hypoesthesia below the T4 dermatome level, dysesthesia to pin prick below the right inguinal level, and motor impairments of both lower
extremities. Motor functions were assessed in five key muscles in the lower extremities, based on the international American Spinal Injury Association (ASIA) scale (Table 1). Anal wink was
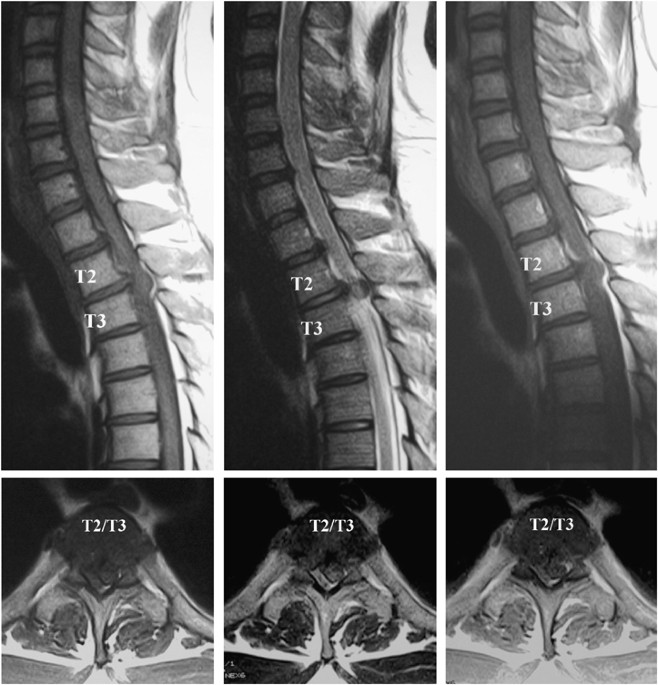
lacking and anal tone was flaccid but anal sphincter motion was preserved (Frankel classification C). Motor and sensory examination of both upper extremities was normal. MR imaging revealed
the localized compression of the thoracic spinal cord at T2–T3 level (Figure 1). Axial MR imaging showed the mass was located postero-laterally and compressed the dural sac. MR imaging with
gadolinium showed slight enhancement of the lesion. Plain X-ray and computerized tomography (CT) of thoracic spine showed no calcification in any intervertebral disc. OPERATION MR imaging
showed the mass was located postero-laterally in the spinal canal and the spinal cord was compressed mainly from the posterior site. Acute idiopathic epidural hematoma, abscess or thoracic
disc herniation could be suspected from the primary clinical and imaging diagnosis. Posterior surgery was thus performed to remove the mass. After laminectomy of T2–T3, hematoma or abscess
could not be detected in the epidural space. However, the terminal end of the sequestrated disc could be detected. The sequestrated disc materials were excised successfully through the right
side of the dura without any damage to it. The extracted herniated mass was a ring-like form and thought to originate from the annulus fibrosis (Figure 2). POSTOPERATIVE COURSE Soon after
the emergency surgery, he had complete relief of his backache. He could stand up without aid on the second postoperative day and he started walking with assistance on the fifth postoperative
day. At 4 weeks after the operation, motor power of both lower extremities had recovered almost completely. He was able to walk without assistance. Sensation also recovered except mild
hypoesthesia below the right inguinal level and he could control his bladder-rectal function well. At 2 months after the operation, he had no complaints in activities in daily living
(Frankel classification E). MR imaging study after surgery did not show a sequestrated mass, but only mild disc bulging at the T2–T3 level. There was no residual spinal cord compression
(Figure 3). DISCUSSION The incidence of symptomatic thoracic disc herniation has been reported to be one per million per year and occurs in only 0.25–0.75% of all intervertebral disc
herniations.1 Our present case, is especially unique in that the upper thoracic disc herniation resulted in acutely progressing paraplegia, and the herniated mass which migrated posteriorly
in the spinal canal, was successfully excised by posterior surgery without fusion. The rarity of thoracic disc herniation probably results from the fact that the thoracic vertebrae are
mechanically stabilized by the rib head joints and, as a result, they avoid dynamic stress.3 Our review of the literature showed that the symptoms of thoracic disc herniation were mainly
_backache_, slowly progressive myelopathy, thoracic nerve radiculopathy and bladder dysfunction.2, 4, 5, 6 Some cases in which acute paraplegia developed from thoracic disc herniations have
been reported;7, 8 however, the present case is unique in that the sequestrated disc migrated posteriorly in the high thoracic spinal canal toward the dorsal side of the dura. The majority
of thoracic disc herniations have been reported to be of the posterior or postero-lateral bulged type.2 Furthermore, some authors had reported that thoracic disc herniation was mostly
associated with radiological calcification of the disc.9, 10, 11 In our case, however, preoperative X-ray, CT scans and macroscopic examination of the herniated disc showed no calcification.
One report in which the thoracic disc herniation was sequestrated to the postero-lateral side of spinal canal could be found.12 In the reported case, X-ray and CT examination showed no
calcification of the herniated disc, similar to our patient. There have been several reports about the surgical procedures for thoracic disc herniations. Stillerman _et al_2 reported four
surgical approaches for thoracic disc herniations: (1) transthoracic, (2) transfacet pedicle-sparing, (3) lateral extracavitary, and (4) transpedicular approaches. Some authors reported that
anterior or antero-lateral discectomy may be the simplest and most effective method for disc excision and relief of spinal cord.4, 13, 14 Furthermore, Vanichkachorn and Vaccaro6 reported
that posterior laminectomy was controversial for the treatment of symptomatic thoracic disc protrusions and recommended that the operative procedure must be chosen carefully among the
anterior, lateral and posterior approaches. The avoidance of the posterior approach might be related to the fact that posterior laminectomy of the thoracic spine characterized by kyphosis
would not successfully lead to decompression of the spinal cord compressed by posterior bulged disc and, furthermore, the spinal cord could be easily damaged when performing disc removal via
posterior laminectomy. In the present case, however, axial MR imaging showed that the mass was located postero-laterally and compressed the dural sac mainly from the posterior site, and
acute idiopathic epidural hematoma or abscess also could be suspected from the primary clinical and imaging diagnosis, therefore posterior surgery was performed. After laminectomy at the
T2–T3 level, the terminal end of the herniated disc material could be detected in the epidural space, so we were able to perform an excision easily, without any damage to the dura. In the
present case, paraplegia developed after antecedent backache lasting several days. The pathogenesis of this thoracic disc herniation could, therefore, be speculated as follows: Preceding
intrinsic disc degeneration due to obesity (height: 177 cm, weight: 100 kg) caused disc budging, then rapid and momentary rise of the intra-discal pressure due to body twisting, etc,
occurred and, as a result, annulus fibrosis ruptured the posterior longitudinal ligament and migrated posteriorly in the spinal canal. Generally, characteristic neurological patterns for
symptomatic thoracic disc herniation are lacking and the localization of pain induced by thoracic disc herniation is sometimes ambiguous. For these reasons, accurate diagnosis of symptomatic
thoracic disc herniation has been reported to be considerably difficult. These facts can lead to delay in diagnosis, which may result in progressive neurological impairments. Previous
reports have shown, however, that postoperative results of acutely developing thoracic disc herniation are generally satisfactory.15 Therefore, appropriate diagnosis and earlier treatment
based on accurate neurological examination and diagnostic imaging, such as MR imaging, can lead to excellent recovery of neurological function. REFERENCES * Arce CA, Dohrmann GJ . Herniated
thoracic disks. _Neurol Clin_ 1985; 3: 383–392. Article CAS Google Scholar * Stillerman CB, Chen TC, Couldwell WT, Zhang W, Weiss MH . Experience in the surgical management of 82
symptomatic herniated thoracic discs and review of the literature. _J Neurosurg_ 1998; 88: 623–633. Article CAS Google Scholar * Oda I, Abumi K, Cunningham BW, Kaneda K, McAfee PC . An
_in vitro_ human cadaveric study investigating the biomechanical properties of the thoracic spine. _Spine_ 2002; 27: 64–70. Article Google Scholar * Caner H, Kilincoglu BF, Benli S,
Altinors N, Bavbek M . Magnetic resonance image findings and surgical considerations in T1–2 disc herniation. _Can J Neurol Sci_ 2003; 30: 152–154. Article CAS Google Scholar * Morgan H,
Abood C . Disc herniation at T1–2. Report of four cases and literature review. _J Neurosurg_ 1998; 88: 148–150. Article CAS Google Scholar * Vanichkachorn JS, Vaccaro AR . Thoracic disk
disease: diagnosis and treatment. _J Am Acad Orthop Surg_ 2000; 8: 159–169. Article CAS Google Scholar * Hamilton MG, Thomas HG . Intradural herniation of a thoracic disc presenting as
flaccid paraplegia: case report. _Neurosurgery_ 1990; 27: 482–484. Article CAS Google Scholar * Chen CF, Chang MC, Liu CL, Chen TH . Acute noncontiguous multiple-level thoracic disc
herniations with myelopathy: a case report. _Spine_ 2004; 29: 157–160. Article Google Scholar * Al-Barbarawi M, Sekhon LH . Management of massive calcified transdural thoracic disk
herniation. _J Clin Neurosci_ 2003; 10: 707–710. Article Google Scholar * Gerster JC, Perez-Sawka I, de Tribolet N . Calcified thoracic herniated disk and chondrocalcinosis. _Schweiz Med
Wochenschr_ 1990; 26: 798–800. Google Scholar * Greco P, Ruosi C, Mariconda M, Piergentili C . Intervertebral disc herniation at D3–4 Case report. _Ital J Orthop Traumatol_ 1989; 15:
377–381. CAS PubMed Google Scholar * Morizane A, Hanakita J, Suwa H, Ohshita N, Gotoh K, Matsuoka T . Dorsally sequestrated thoracic disc herniation – case report. _Neurol Med Chir
(Tokyo)_ 1999; 39: 769–772. Article CAS Google Scholar * Okada Y, Shimizu K, Ido K, Kotani S . Multiple thoracic disc herniations: case report and review of the literature. _Spinal Cord_
1997; 35: 183–186. Article CAS Google Scholar * Turgut M . Spinal cord compression due to multivel thoracic disc herniation: surgical decompression using a ‘combined’ approach. A case
report and review of the literature. _J Neurosurg Sci_ 2000; 44: 53–59. CAS PubMed Google Scholar * Rapport RL, Hillier D, Scearce T, Ferguson C . Spontaneous intracranial hypotension
from intradural thoracic disc herniation. Case report. _J Neurosurg_ 2003; 98: 282–284. PubMed Google Scholar Download references AUTHOR INFORMATION AUTHORS AND AFFILIATIONS * Department
of Orthopaedic Surgery, Japan Labour, Health and Welfare Organization, Spinal Injuries Center, Iizuka-shi, Fukuoka, Japan S Sasaki, K Kaji & K Shiba Authors * S Sasaki View author
publications You can also search for this author inPubMed Google Scholar * K Kaji View author publications You can also search for this author inPubMed Google Scholar * K Shiba View author
publications You can also search for this author inPubMed Google Scholar RIGHTS AND PERMISSIONS Reprints and permissions ABOUT THIS ARTICLE CITE THIS ARTICLE Sasaki, S., Kaji, K. &
Shiba, K. Upper thoracic disc herniation followed by acutely progressing paraplegia. _Spinal Cord_ 43, 741–745 (2005). https://doi.org/10.1038/sj.sc.3101781 Download citation * Published: 05
July 2005 * Issue Date: 01 December 2005 * DOI: https://doi.org/10.1038/sj.sc.3101781 SHARE THIS ARTICLE Anyone you share the following link with will be able to read this content: Get
shareable link Sorry, a shareable link is not currently available for this article. Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative KEYWORDS * thoracic
disc herniation * acutely progressing paraplegia * upper thoracic
Trending News
Access to this page has been deniedYour browser appears to have Javascript disabled.For instructions on how to enable Javascript please click here.If you h...
Japanese lessons: is liz truss right to turn to tokyo to curb inflation? | thearticleThe bookies favourite to be the UK’s next Prime Minister, Liz Truss, has gone on record saying that, in her opinion, the...
City seeks public input on designThe city recently equipped a group of students and a cross-section of Ventura residents with disposable cameras and aske...
Star wars is a religion that primes us for war and violence$1 That’s what it cost 14-year-old me to get into the 1977 _Star Wars_ premiere. $10 That’s how much I eventually stole ...
The spirit of waldorf educationFor a small but growing number of critics, the allure of public Waldorf schools is profoundly deceptive. The K-8 Yuba Ri...
Latests News
Upper thoracic disc herniation followed by acutely progressing paraplegiaABSTRACT STUDY DESIGN: Case report. OBJECTIVE: To report a rare thoracic intervertebral disc herniation followed by acut...
Carbon–carbon bond cleavage for a lignin refineryABSTRACT Carbon–carbon bonds, ubiquitous in lignin, limit monomer yields from current depolymerization strategies, which...
Effects of rice-based and wheat-based diets on bowel movements in young korean women with functional constipationABSTRACT BACKGROUND Although several studies have reported the effects that dietary fiber intake from different types of...
Life in the slow lane | Nature Reviews MicrobiologyAccess through your institution Buy or subscribe When conditions are unfavourable, for example, owing to nutrient limita...
Plight of migrant laborers killed, held hostage in middle east exposes israel’s reliance on overseas workforceAn Indian laborer in Israel was killed and several other migrant workers injured on March 4, 2024, in a missile attack l...